
Celiac Disease Testing - CAM 315
Description:
Celiac disease is a hereditary, chronic autoimmune disorder triggered by the ingestion of gluten, a protein found in wheat, rye, and barley. When an individual with celiac disease ingests gluten, the body mounts an immune response that attacks the small intestine. These attacks lead to damage on the villi within the small intestine, inhibiting nutrient absorption (CDF, 2018).
RegulatoryStatus
The Quanta Lite Celiac Screen ELISA test for tissue transglutaminase/gliadin and the Quanta Lite Celiac DGP Screen by Inova Diagnostics, Inc. were approved by the FDA on Jan. 28, 1999 and Dec. 13, 2006, respectively. Quanta Plex Celiac IgA and IgG profiles by Inova Diagnostics, Inc. were approved on March 14, 2007 and June 20, 2007.
EliA Celikey IgG for use with the EliA Celikey IgG Immunoassay by Phadia US, Inc. was approved by the FDA on Dec. 26, 2006.
The FIDIS Celiac on the FIDS Analyser and FIDIS CELIAC kit by Biomedical Diagnostics S.A. were approved by the FDA on Sept. 24, 2004 and March 29, 2006, respectively.
The IMMULISA CELIAC ELISA testing systems for gliadin IgA/IgG and TTG IgA/IgG by IMMCO Diagnostics, Inc. were approved on Feb. 4, 2010 and March 10, 2010. IMMCO’s IMMULISA enhanced celiac fusion (TTG/DGP) IgA/IgG antibody ELISA system was approved on Oct. 25, 2013.
Bio-Rad Laboratories’ Bioplex 2200 Celiac IgA IgG kits were approved on Sept. 19, 2013. The IgX Plex Celiac qualitative assay and Ig Plex Celiac DG panel by SQI diagnostics systems, Inc. were approved by the FDA on June 2, 2011 and Nov. 6, 2014, respectively.
SQI Diagnostics received FDA clearance for the Ig_plex Celiac DGP which detects IgA and IgG antibodies to deamidated gliadin peptide (DGP) and tissue transglutaminase (tTG) in human serum. This was approved by the FDA on Nov. 6, 2014 (FDA, 2014).
Inova Diagnostics received FDA clearance on June 16, 2021 for the Aptiva Celiac Disease IgA Reagent, which is an “immunoassay utilizing particle-based multi-analyte technology for the semi-quantitative determination of anti-tissue transglutaminase IgA autoantibodies and anti-deamidated gliadin peptide IgA antibodies in human serum.” It can be used to diagnose celiac disease and dermatitis herpetiformis (FDA, 2021b).
No nucleic acid-based test solely for celiac disease has been approved by the FDA as of July 2019. The FDA has approved the direct-to-consumer panel test by 23andme that includes a single nucleotide polymorphism in HLA-DQA1 (FDA, 2017).
A search of the FDA database on July 9, 2021 using the term “celiac” yielded 18 results (FDA, 2021a). Additionally, many labs have developed specific tests that they must validate and perform in house. These laboratory-developed tests (LDTs) are regulated by the Centers for Medicare & Medicaid Services (CMS) as high-complexity tests under the Clinical Laboratory Improvement Amendments of 1988 (CLIA ’88). As an LDT, the U.S. Food and Drug Administration has not approved or cleared this test; however, FDA clearance or approval is not currently required for clinical use.
Policy:
Application of coverage criteria is dependent upon an individual’s benefit coverage at the time of the request.
- For individuals with signs and symptoms of celiac disease (See Note 1), serologic testing with the IgA anti-tissue transglutaminase (TTG) and the total IgA test for the diagnosis of celiac disease is considered MEDICALLY NECESSARY.
- For individuals at risk for celiac disease (See Note 1), when IgA anti-TTG is negative or weakly positive, testing for IgA endomysial antibodies is considered MEDICALLY NECESSARY.
- For individuals with clinical suspicion of celiac disease (See Note 1) with an IgA deficiency, testing for IgG endomysial antibodies, IgG deamidated gliadin peptide, or IgG TTG is considered MEDICALLY NECESSARY.
- For children under 2 years of age with a clinical suspicion of celiac disease (See Note 1) and in those over 2 years of age as a substitute for anti-TTG testing, testing for IgA and IgG antibodies to deamidated gliadin peptides is considered MEDICALLY NECESSARY.
- Genetic testing for HLA DQ2 and is considered NOT MEDICALLY NECESSARY for:
- Symptomatic individuals for whom other testing is undiagnostic; OR
- Symptomatic individuals with positive serology tests who are unable to undergo biopsy evaluation
- For confirmation of celiac disease in individuals at high risk for celiac disease, regardless of the result of celiac disease serology testing, biopsy of the small intestine is considered MEDICALLY NECESSARY.
- Rapid antigen point-of-care testing for anti-TTG DOES is considered NOT MEDICALLY NECESSARY.
- Panel testing, multiplex, or multi-analyte testing (for more than two analytes) for the diagnosis or evaluation of celiac disease is considered NOT MEDICALLY NECESSARY.
The following does not meet coverage criteria due to a lack of available published scientific literature confirming that the test(s) is/are required and beneficial for the diagnosis and treatment of a patient’s illness.
- Testing for anti-reticulin antibodies is considered NOT MEDICALLY NECESSARY for the diagnosis of celiac disease.
- Testing of stool or saliva samples for the evaluation of celiac disease is considered NOT MEDICALLY NECESSARY.
- Serologic testing using an HLA-DQ-gluten tetramer-based assay, including flow cytometry-based HLA-DQ-gluten tetramer assays, is considered NOT MEDICALLY NECESSARY.
NOTE 1: Signs and symptoms of celiac disease may include, but are not limited to, the following: unexplained chronic or intermittent diarrhea; unexplained weight loss; unexplained chronic or intermittent abdominal pain or bloating; recurrent nausea or vomiting; unexplained iron deficiency anemia; unexplained vitamin B12 or folate deficiency; unexplained liver transaminase elevations; autoimmune hepatitis; dermatitis herpetiformis; Type 1 diabetes; intestinal blockages; unexplained subfertility or miscarriage; unexplained osteoporosis, osteomalacia, or low bone density; and/or primary biliary cirrhosis. Individuals with Down syndrome, Turner syndrome, or Willams-Beuren syndrome are also at high risk for celiac disease. Additionally, in pediatric patients, fatty stools, delayed puberty, amenorrhea, failure to thrive, stunted growth, and/or short stature may also be associated with celiac disease (Husby et al., 2020; NICE, 2022; NIDDK, 2016).
Rationale
Celiac disease (CD) is an autoimmune disease which occurs due to the body’s unfavorable response after the ingestion of gluten. In particular, the body’s immune system attacks the small intestine, leading to damage and inhibiting nutrient absorption (CDF, 2018). The clinical presentation of CD is varied and age dependent. In children, failure to thrive, malnutrition, diarrhea, abdominal pain, and distension are common. In adults, abdominal pain, diarrhea or constipation, bloating, and excessive gas are frequent symptoms. Other gastrointestinal symptoms include unexpected weight loss and distension (Kelly, 2022). CD is more common in females than males (Jansson-Knodell et al., 2019), and a high prevalence of cases are often found in first degree relatives of CD patients, highlighting genetic aspects of the disease (Nellikkal et al., 2019). Currently, the only treatment for CD is to maintain a gluten-free diet to ameliorate symptoms and improve the quality of life (Caio et al., 2019).
The National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK, 2020) provides the following statistics for CD:
- About 2 million Americans have CD.
- About 1% of people worldwide have CD.
- The majority of people are undiagnosed .
- CD can affect all races, but is present at a higher rate in Caucasians.
- CD can affect both genders, but a higher rate is identified in females.
- CD is more common among people with chromosomal disorders like Down syndrome, Turner syndrome, and Williams syndrome.
- Patients with CD are at risk for Addison’s disease, Hashimoto’s disease, selective IgA deficiency, primary biliary cholangitis, and Type 1 diabetes.
CD has a strong genetic component. The two primary genetic factors for CD susceptibility are the human leukocyte antigen (HLA)-DQ2 and DQ8 alleles (Brown et al., 2019). These genes highlight the role of T cells and the immune response in CD (Tye-Din et al., 2018). Approximately 90-95% of CD patients have the HLA-DQ2 protein encoded by the HLA-DQA1*05 and DQB1*02 alleles. The remaining CD patients have mutations in the HLA-DQ8 protein encoded by the HLA-DQA1*03 and DQB1*03:02 alleles. Stankovic et al. (2014) noted that the absence of susceptible HLA-DQ genotypes makes CD “very unlikely, close to 100%.” However, the use of genotyping in diagnosing CD is not without controversy. Paul et al. (2017) report that 25 – 40% of white Caucasians are positive for the HLA-DQ2/DQ8 haplotype but that only 0.1 – 1% of the population will develop CD. They also note that the European guidelines released in 2012 recommend genotyping for HLA-DQ2/DQ8 in children with very high anti-TTG titers, but the authors recommend that “HLA-DQ2/DQ8 testing must not be done to 'screen' or 'diagnose' children” with CD (Paul et al., 2017).
Antibodies for the assessment of CD generally fall into one of two categories: autoantibodies (tTG-IgA, anti-endomysial antibody [EMA-IgA]) or antibodies targeting gliadin (DGP-IgA or IgG, antigliadin antibody (AGA)-IgA or IgG). Endomysial antibodies bind to tissue transglutaminase and produce a characteristic staining pattern. Similarly, anti-endomysial antibodies bind to tTG-2, another tissue transglutaminase. The other category of celiac antibodies involve gliadin, which is a component of gluten. Traditional antigliadin antibody tests (AGA-IgA, AGA-IgG) yielded a false positive rate of up to 20%, so they have been replaced with a deamidated gliadin peptide (DGP) (Kelly, 2022).
Genetic testing for HLA DQ2 and DQ8 may also be used to confirm a CD diagnosis. Serologic and histologic HLA-DQ testing requires the patient to be on a gluten-containing diet, which can be a disadvantage to testing. Recently, testing methods for HLA-DQ-gluten tetramer-based assays using flow-cytometry have been developed; these tests can accurately determine whether the patient is on a gluten-containing or gluten-free diet. The assay has a reported 97% sensitivity and 95% specificity for patients on a gluten-free diet as compared to controls (patients without CD) (Sarna et al., 2018). The authors conclude, “This test would allow individuals with suspected celiac disease to avoid gluten challenge and duodenal biopsy, but requires validation in a larger study” (Sarna et al., 2018).
Point of care tests, such as the Simtomax®, have been developed, which detects IgA and IgG antibodies against deamidated gliadin peptides (DGP) and provides a response in just ten minutes (Arenda, 2020). There are also direct-to-consumer (DTC) tests for CD. The FDA-approved 23andme panel includes CD. This test detects a single nucleotide polymorphism in HLA-DQA1 (FDA, 2017).
Clinical Utility and Validity
Olen et al. (2012) evaluated the diagnostic performance and actual costs in clinical practice of immunoglobulin (Ig)G/IgA DGP (deamidated gliadin peptide antibodies) as a complement to IgA-TTG for the diagnosis of pediatric CD. The authors identified 278 children with CD that received a duodenal biopsy. Sensitivity and specificity for tTG were 94% and 86% respectively, but corresponding values for DGP were 91% and 26%. Positive predictive values were 88% for tTG and 51% for DGP. The authors concluded that for diagnosing CD, tTG is superior to DGP, even in children younger than 2 years. Further, combining tTG and DGP does not provide a better trade-off between number of missed cases of CD, number of unnecessary duodenal biopsies, and cost than utilizing tTG alone (Olen et al., 2012).
Sakly et al. (2012) evaluated the usefulness of anti-DGP antibodies (a-DGP) in the diagnosis of CD. The study included 103 untreated CD patients of all ages and 36 CD patients under a gluten-free diet. The specificity of a-DGP was 93.6% for IgG and 92% for IgA as compared to the 100% for each by anti-endomysium antibodies (AEA) and tTG. The authors concluded that the findings of this study showed “that a-DGP increases neither the sensitivity nor the specificity of AEA and AtTG [anti-tissue transglutaminase antibodies]” (Sakly et al., 2012).
Bufler et al. (2015) evaluated the diagnostic performance of three serological tests for CD. A total of 91 children with CD contributed 411 sera samples and were compared to 98 healthy controls. Transglutaminase type 2(TG2)-IgA, deamidated gliadin peptide (DGP)-IgG, and DGP-IgA were measured. The sensitivity for diagnosis was high for TG2-IgA and DGP-IgG (> 90%) but lower for DGP-IgA. Specificity was >97% for all three. Non-adherence to a gluten-free diet was best indicated by positive TG2-IgA. The authors concluded that “combined testing for TG2-IgA and DGP-IgG does not increase the detection rate of CD in IgA competent children compared to TG2-IgA only” (Bufler et al., 2015).
Silvester et al. (2017) performed a meta-analysis to evaluate the “sensitivity and specificity of tTG IgA and EMA [endomysial antibody] IgA assays in identifying patients with celiac disease who have persistent villous atrophy despite a gluten-free diet (GFD).” The authors identified 26 studies for inclusion. The assays were found to have high specificity for identifying patients with persistent villous atrophy (0.83 for tTG IgA, 0.91 for EMA IgA, but with low sensitivity (0.50 for tTG IgA, 0.45 for EMA IgA). No significant difference was seen between pediatric and adult patients. The authors concluded that “we need more-accurate non-invasive markers of mucosal damage in children and adults with celiac disease who are following a GFD” (Silvester et al., 2017).
A report by Selleski et al. (2018) shows that only some of the DQ2/DQ8 alleles were significantly different between pediatric CD patients and pediatric non-CD patients. A total of 97% of the CD patients were positive for at least either DQ2 or DQ8; however, 29.9% of the non-CD patients were also positive for DQ2. In fact, “No significant association was found between DQ2.2 variant and celiac disease in the studied population (Selleski et al., 2018).” Previously, high regard had been given to DQ2.2 variant as being a predisposing variant for CD (Mubarak et al., 2013). Finally, a rapid nucleic acid amplification test using multiplex ligation-dependent probe amplification (MLPA) to detect HLA-DQ2.2, HLA-DQ2.5, and HLA-DQ8 has been developed with a reported 100% specificity for those particular genotypes (Vijzelaar et al., 2016), but this test has not been FDA-approved for use in the United States.
Bajor et al. (2019) performed a meta-analysis focusing on the association between the HLA-DQB1*02 gene doses and the characteristics of CD. The authors identified 24 studies for inclusion in the review and observed that homozygosity of the DQB1*02 allele led to more frequent classical CD (odds ratio [OR] 1.758). The gene dosing effect was more prominent in children (OR: 2.082). Atrophic histology (Marsh grade 3) was more prevalent with a double dose compared to a zero dose (OR: 2.626). No gene dosing effect was seen with diarrhea, age at diagnosis, severity of villous atrophy, or type 1 diabetes. The authors concluded that “A double dose of HLA-DQB1*02 gene seems to predispose patients to developing classical CD and villous atrophy. Risk stratification by HLA-DQB1*02 gene dose requires further clarification due to the limited available evidence” (Bajor et al., 2019).
Tangermann et al. (2019) completed a prospective study which included 1055 patients all tested for CD with the Simtomax point of care test. The Simtomax detects IgA and IgG antibodies against deamidated gliadin peptides (DGP). All results were compared to the gold standard: histologic analysis of duodenal biopsies. Of all patients who participated in this study, the overall CD prevalence was identified at 4.1%; the Simtomax identified CD with a 79% sensitivity, 94% specificity, 37% positive predictive value, and 99% negative predictive value (Tangermann et al., 2019). When the adult (n = 888) and pediatric (n = 167) patients were analyzed separately, the Simtomax was found to identify CD with 100% sensitivity and 95% specificity in adults, and 72% sensitivity in children; the authors note that the Simtomax test detected CD with a lower sensitivity than expected (Tangermann et al., 2019).
Profaizer et al. (2020) conducted a study to “evaluate the feasibility of using NGS-based [next-generation sequencing] HLA-B and DQ genotyping for clinical HLA disease association testing and provide direct comparison with the currently used clinical tests, including SSOP [sequence-specific oligonucleotide probe] genotyping, and real-time PCR [polymerase chain reaction] with melting chain analysis.” The researchers focused on HLA alleles related to celiac disease, ankylosing spondylitis, abacavir hypersensitivity, carbamazepine hypersensitivity, and allopurinol hypersensitivity. With regards to CD and from 24 samples tested, there was a discrepancy with the DQB1*03:40 allele with SSOP, real-time PCR, and NGS, but overall, with the different HLA-correlations the data has shown “HLA typing by NGS is superior to the existing clinical methods for identifying HLA alleles associated with disease or drug hypersensitivity and offers a viable approach for high volume clinical diagnostic laboratories,” continuing to demonstrate the clinical utility of NGS and HLA-testing for CD (Profaizer et al., 2020).
Gould et al. (2021) evaluated CD serologic testing in asymptomatic patients with Type 1 diabetes using immunoglobulin A anti-tissue transglutaminase, as there is an increased risk of type 1 diabetes among CD and vice versa. From screening 2,353 patients, the assay with IgA anti-tissue transglutaminase had a positive predictive value of 85.9% when referenced upper limit of normal and had a sensitivity and specificity of 100% and 38%, respectively. This study indicated the need for thresholds for diagnostic evaluation to be population-specific (i.e. to type 1 diabetics), and not taken from the overall population due to the increased risk (Gould et al., 2021).
Schuppan et al. (2021) assessed the efficacy and safety of a 6-week treatment with ZED1227, a selective oral transglutaminase 2 inhibitor, at three dose levels compared with placebo, in adults with well-controlled celiac disease who underwent a daily gluten challenge. Their primary endpoint was the attenuation of gluten-induced mucosal damage, measured by the ratio of villus height to crypt death. For this study, 41 patients were assigned to the 10-mg ZED1227 group, 41 patients were assigned to the 100-mg group, and 40 patients were assigned to the placebo group. Each had adequate duodenal-biopsy samples for the assessment of the overall endpoint. “The estimated difference from placebo in the change in the mean ratio of villus height to crypt depth from baseline to week 6 was 0.44 (95% confidence interval [CI], 0.15 to 0.73) in the 10-mg group (P = 0.001), 0.49 (95% CI, 0.20 to 0.77) in the 50-mg group (P < 0.001), and 0.48 (95% CI, 0.20 to 0.77) in the 100-mg group (P < 0.001). The estimated differences from placebo in the change in intraepithelial lymphocyte density were -2.7 cells per 100 epithelial cells (95% CI, -7.6 to 2.2) in the 10-mg group, -4.2 cells per 100 epithelial cells (95% CI, -8.9 to 0.6) in the 50-mg group, and -9.6 cells per 100 epithelial cells (95% CI, -14.4 to -4.8) in the 100-mg group.” The authors concluded that treatment with ZED1227 attenuated gluten-induced duodenal mucosal damage in patients with celiac disease. (Schuppan et al., 2021).
American College of Gastroenterology (ACG)
The ACG recommends testing for CD in the following scenarios (Rubio-Tapia et al., 2013):
- “Patients with symptoms, signs, or laboratory evidence suggestive of malabsorption, such as chronic diarrhea with weight loss, steatorrhea, postprandial abdominal pain and bloating, should be tested for CD. (Strong recommendation, high level of evidence)”
- “Patients with symptoms, signs, or laboratory evidence for which CD is a treatable cause should be considered for testing for CD. (Strong recommendation, moderate level of evidence)”
- “Patients with a first-degree family member who has a confirmed diagnosis of CD should be tested if they show possible signs or symptoms or laboratory evidence of CD. (Strong recommendation, high level of evidence)”
- “Patients with type I diabetes mellitus should be tested for CD if there are any digestive symptoms, or signs, or laboratory evidence suggestive of celiac disease. (Strong recommendation, high level of evidence)”
- “Celiac disease should be sought among the explanations for elevated serum aminotransferase levels when no other etiology is found, (Strong recommendation, high level of evidence)”
- “Consider testing of asymptomatic relatives with a first-degree family member who has a confirmed diagnosis of CD (Conditional recommendation, high level of evidence)”
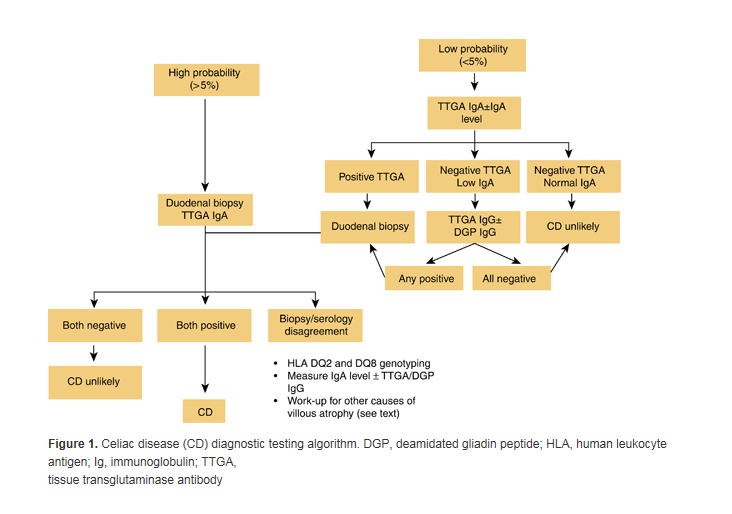
The ACG guidelines indicate that “Immunoglobulin A (IgA) anti-tissue transglutaminase (TTG) antibody is the preferred single test for detection of CD in individuals over the age of 2 years.” Also, if there is “a high probability of CD wherein the possibility of IgA deficiency is considered, total IgA should be measured.” Additionally, “an alternative approach is to include both IgA and IgG-based testing, such as IgG-deamidated gliadin peptides (DGPs), in these high-probability patients.” In those patients with low or deficient IgA, the ACG recommends “IgG-based testing (IgG DGPs and IgG TTG).” The guidelines also indicate that all serological testing should be done while the individual is on a gluten-containing diet.
Intestinal biopsy is recommended by the ACG for individuals with positive serology testing and for those with a clinical presentation consistent with CD, “even if the serologies are negative.”
Although antibodies directed against native gliadin are not recommended for the primary detection of CD,” the ACG notes that “when screening children younger than 2 years of age for CD, the IgA TTG test should be combined with DGP (IgA and IgG).”
With regard to HLA-DQ2/DQ8 genotype testing, the ACG recommends that it “should not be used routinely in the initial diagnosis of CD” but rather “should be used to effectively rule out the disease in selected clinical situations” such as, “equivocal small-bowel histological finding (Marsh I – II) in seronegative patients; evaluation of patients on a GFD in whom no testing for CD was done before GFD; patients with discrepant celiac-specific serology and histology; patients with suspicion of refractory CD where the original diagnosis of celiac remains in question; or patients with Down’s syndrome. … Because HLA-DQ2 is present in approximately 25% – 30% of the white population, testing for CD with either HLA-DQ type is not useful because the PPV is only about 12%.” Concerning HLA typing, “HLA typing, and histological response may help to rule out or confirm the diagnosis of CD in patients with sero-negative CD.”
The ACG does not recommend stool or salivary testing, indicating that are not validated for use in the diagnosis of CD.
The ACG advocates monitoring of adherence to a gluten-free diet, based on “a combination of history and serology.” Additionally, “upper endoscopy with intestinal biopsies is recommended for monitoring in cases with lack of clinical response or relapse of symptoms despite a GFD.”
Celiac Disease Diagnostic Testing Algorithm (Rubio-Tapia et al., 2013)
American Gastroenterological Association (AGA)
Relative to ongoing monitoring of individuals with celiac disease, the AGA recommends periodic serologic testing.
The AGA published an update on CD testing in 2019. Their new “best practice advice” is as follows:
- “Best Practice Advice 1: Serology is a crucial component of the detection and diagnosis of CD, particularly tissue transglutaminase–immunoglobulin A (TG2-IgA), IgA testing, and less frequently, endomysial IgA testing.”
- “Best Practice Advice 2: Thorough histological analysis of duodenal biopsies with Marsh classification, counting of lymphocytes per high-power field, and morphometry is important for diagnosis as well as for differential diagnosis.”
- “Best Practice Advice 2a: TG2-IgA, at high levels (> ×10 upper normal limit) is a reliable and accurate test for diagnosing active CD. When such a strongly positive TG2-IgA is combined with a positive endomysial antibody in a second blood sample, the positive predictive value for CD is virtually 100%. In adults, esophagogastroduodenoscopy (EGD) and duodenal biopsies may then be performed for purposes of differential diagnosis.”
- “Best Practice Advice 3: IgA deficiency is an infrequent but important explanation for why patients with CD may be negative on IgA isotype testing despite strong suspicion. Measuring total IgA levels, IgG deamidated gliadin antibody tests, and TG2-IgG testing in that circumstance is recommended.”
- “Best Practice Advice 4: IgG isotype testing for TG2 antibody is not specific in the absence of IgA deficiency.”
- “Best Practice Advice 5: In patients found to have CD first by intestinal biopsies, celiac-specific serology should be undertaken as a confirmatory test before initiation of a gluten-free diet (GFD).”
- “Best Practice Advice 6: In patients in whom CD is strongly suspected in the face of negative biopsies, TG2-IgA should still be performed and, if positive, repeat biopsies might be considered either at that time or sometime in the future.”
- “Best Practice Advice 7: Reduction or avoidance of gluten before diagnostic testing is discouraged, as it may reduce the sensitivity of both serology and biopsy testing.”
- “Best Practice Advice 8: When patients have already started on a GFD before diagnosis, we suggest that the patient go back on a normal diet with 3 slices of wheat bread daily preferably for 1 to 3 months before repeat determination of TG2-IgA.”
- “Best Practice Advice 9: Determination of HLA-DQ2/DQ8 has a limited role in the diagnosis of CD. Its value is largely related to its negative predictive value to rule out CD in patients who are seronegative in the face of histologic changes, in patients who did not have serologic confirmation at the time of diagnosis, and in those patients with a historic diagnosis of CD; especially as very young children before the introduction of celiac-specific serology” (Husby et al., 2019).
European Society for Pediatric Gastroenterology, Hepatology, and Nutrition (ESP-GHAN)
Updated and expanded evidence-based guidelines for diagnosing CD were published in 2020 by the ESP-GHAN. The following recommendations were included (Husby et al., 2020):
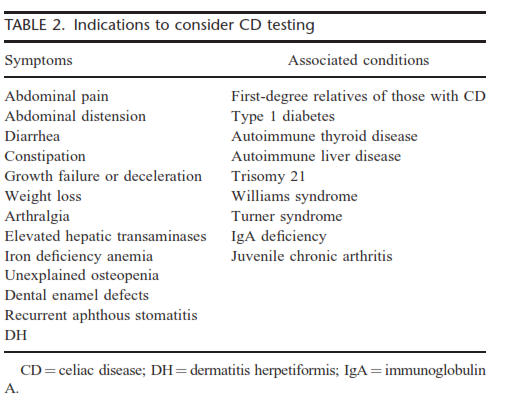
- “We recommend considering testing for CD in children and adolescents with symptoms, signs and conditions shown in Table 2.”
- Signs and symptoms in Table 2 include:
- “Gastrointestinal: chronic or intermittent diarrhea, chronic constipation not responding to usual treatment, chronic abdominal pain, distended abdomen, recurrent nausea, recurrent vomiting.
- Extraintestinal symptoms: weight loss, failure to thrive, stunted growth/short stature, delayed puberty, amenorrhea, irritability, chronic fatigue, neuropathy, arthritis/arthralgia, chronic iron-deficiency anemia, decreased bone materialization (osteopenia/osteoporosis), repetitive fractures, recurrent aphthous stomatitis, dermatitis herpetiformis-type rash, dental enamel defects, abnormal liver biochemistry.
- Specific conditions: first degree relatives with CD, autoimmune conditions: TIDM, thyroid disease, liver disease, Down syndrome, Turner syndrome, Williams-Beuren syndrome, IgA deficiency.”
- Signs and symptoms in Table 2 include:
- “HLA typing does not add to the certainty of the diagnosis if the other criteria for CD diagnosis are fulfilled. Testing for HLA DQ2 and DQ8 may be useful in other circumstances. If no risk alleles are found, CD is unlikely. We recommend that HLA typing is not required in patients with positive TGA-IgA, if they qualify for CD diagnosis with biopsies or if they have high serum TGA-IgA (≥ 10× ULN) and EMA-IgA positivity. If a patient tests negative for HLA DQ2 and DQ8, the risk of CD is very low, while a positive result does not confirm the diagnosis.”
- “Recent studies suggest that the no-biopsy approach to diagnose CD can be applied in asymptomatic children. In asymptomatic children, however, the PPV of high TGA-IgA ≥ 10× ULN may be lower than in symptomatic children, which needs to be considered during the decision-making process. We give a conditional recommendation that, taking available evidence into account, CD can be diagnosed without duodenal biopsies in asymptomatic children, using the same criteria as in patients with symptoms. We recommend that the decision whether or not to perform diagnostic duodenal biopsies should be made during a shared decision-making process together with the parent(s) and, if appropriate, with the child.”
- “The three specific coeliac antibodies (TGA-IgA, EMA-IgA, DGP-IgG) show different performance. TGA-IgA scored highest by a comparison of assay accuracy and is therefore regarded as the most appropriate primary test for CD in the diagnostic work up of children with suspected CD. We recommend that in subjects with normal serum IgA values for age, TGA-IgA should be used as the initial test regardless of age.”
- “We recommend testing for total IgA and TGA-IgA as initial screening in children with suspected CD. In patients with low total IgA concentrations, an IgG-based test (DGP, EMA, or TGA) should be performed as a second step. Testing for EMA, DGP or AGA antibodies (IgG and IgA) as initial screening in clinical practice is not recommended.”
- “We recommend that for CD diagnosis without biopsies, TGA-IgA serum concentration of at least 10× ULN should be obligatory. Only antibody tests with proper calibrator curve-based calculation, and having the 10× ULN value within their measurement range, should be used. We recommend against omitting biopsies in IgA-deficient cases with positive IgG-based serological tests.”
- “We recommend that in children with TGA ≥ 10× ULN, and parents/patient agreement to the no-biopsy approach, the CD diagnosis should be confirmed by a positive EMA-IgA test in a second blood sample.”
- “At least 4 biopsies from the distal duodenum and at least 1 from the duodenal bulb should be taken for histology assessment during a gluten-containing diet. Reading of biopsies should be performed on optimally orientated biopsies. A villous to crypt ratio of < 2 indicates mucosal lesions. In cases of discordant results between TGA-IgA results and histopathology, re-cutting of biopsies and/or second opinion from an experienced pathologist should be requested (Husby et al., 2020).”
In 2012, the European Society for Pediatric Gastroenterology, Hepatology, and Nutrition (ESP-GHAN) recommended that CD testing be considered for: “children and adolescents with the otherwise unexplained symptoms and signs of chronic or intermittent diarrhoea, failure to thrive, weight loss, stunted growth, delayed puberty, amenorrhoea, iron-deficiency anaemia, nausea or vomiting, chronic abdominal pain, cramping or distension, chronic constipation, chronic fatigue, recurrent aphthous stomatitis (mouth ulcers), dermatitis herpetiformis–like rash, fracture with inadequate traumas/osteopenia/osteoporosis, and abnormal liver biochemistry.” Testing should also be offered to “asymptomatic children and adolescents with an increased risk for CD such as type 1 diabetes mellitus (T1DM), Down syndrome, autoimmune thyroid disease, Turner syndrome, Williams syndrome, selective immunoglobulin A (IgA) deficiency, autoimmune liver disease, and first-degree relatives with CD (Husby et al., 2012).”
ESP-GHAN recommends that “the initial test be IgA class anti-TG2 from a blood sample. If total serum IgA is not known, then this also should be measured.” If the individual has humoral IgA deficiency, “at least 1 additional test measuring IgG class CD-specific antibodies should be done (IgG anti-TG2, IgG anti-DGP or IgG EMA.” They also note that “tests measuring antibodies against DGP may be used as additional tests in patients who are negative for other CD-specific antibodies but in whom clinical symptoms raise a strong suspicion of CD, especially if they are younger than 2 years,” and “tests for the detection of IgG or IgA antibodies against native gliadin peptides (conventional gliadin antibody test) should not be used for CD diagnosis.” They also indicate that “tests for the detection of antibodies of any type in faecal samples should not be used.”
For individuals with “severe symptoms and a strong clinical suspicion of CD” and negative serology testing, “small intestinal biopsies and HLA-DQ testing are recommended.”
With regard to the evaluation of asymptomatic children and adolescents with CD-associated conditions, ESP-GHAN recommends HLA testing “should be offered as the first line test,” due to its high negative predictive value. “If the patient is DQ8 and/or DQ2 positive, homozygous for only the bchains of the HLA-DQ2 complex (DQB1_0202), or HLA testing is not done, then an anti-TG2 IgA test and total IgA determination should be performed, but preferably not before the child is 2 years old. If antibodies are negative, then repeated testing for CD-specific antibodies is recommended (Husby et al., 2012).”
ESP-GHAN also recommends that in asymptomatic individuals at increased genetic risk for CD “duodenal biopsies with the demonstration of an enteropathy should always be part of the CD diagnosis.” As an initial step, “it is recommended that the more specific test for EMA be performed. If the EMA test is positive, then the child should be referred for duodenal biopsies. If the EMA test is negative, then repeated serological testing on a normal gluten-containing diet in 3 to 6 monthly intervals is recommended (Husby et al., 2012).” Testing of infants, as with all serologic testing for CD, should be done only when the individual is on a gluten-containing diet.
North American Society for Pediatric Gastroenterology, Hepatology, and Nutrition
NASPGHAN updated their recommendations in 2015 (published in 2016) for gluten-related disorders, including CD, wheat allergy (WA), and nonceliac gluten sensitivity (NCGS). Concerning who should be tested for gluten-related disorders, “Children with symptoms consistent with gluten-related disorders, or who have self-identified relief of symptoms when avoiding gluten, should undergo testing for CD and/or WA before the elimination of dietary gluten. CD should be an early consideration in those with typical gastrointestinal symptoms such as chronic diarrhea, abdominal pain, distension, and weight loss.” The table below outlines their recommendations for considering CD testing:
“Children belonging to groups known to be at increased risk for CD may initially have no symptoms, or very minor symptoms, despite having intestinal histologic changes that are characteristic for CD. Included in these groups are first-degree relatives of an index case, people with trisomy 21, Turner syndrome, Williams syndrome, and IgA deficiency, and those with other autoimmune conditions (Hill et al., 2016).”
For initial testing, they recommend the TTG-IgA antibody test due to its reliability and cost-effectiveness. They note that co-testing for serum IgA can be performed to “identify those who have selective IgA deficiency”; however, “use of a panel of antibodies instead of a single tTG-IgA test is not recommended. Although this approach may be associated with a marginal increase in the sensitivity of the test, it decreases the specificity and significantly increases the costs (Hill et al., 2016).” Testing for serum antibodies against gliadin is less sensitive, reliable, and specific as compared to TTG and EMA.
They do not recommend genetic testing for HLA variants as an initial diagnostic test or screening for CD since up to 40% of the general population contains one of the variant alleles. “Testing for HLA-DQ2/8 is best reserved for patients in whom there is a diagnostic dilemma, such as when there is a discrepancy between the serological and histologic findings or when a GFD [gluten-free diet] has been started before any testing (Hill et al., 2016).”
They do not recommend the use of rapid, point-of-care tests for TTG since these tests do not allow for the quantitative analysis of the antibody.
National Institute for Health and Care Excellence (NICE)
In 2022, NICE published guidance on diagnosing CD. These guidelines state that serological testing should be offered to “people with any of the following: persistent unexplained abdominal or gastrointestinal symptoms, faltering growth, prolonged fatigue, unexpected weight loss, severe or persistent mouth ulcers, unexplained iron, vitamin B12 or folate deficiency, type 1 diabetes, at diagnosis, autoimmune thyroid diseases, at diagnosis, irritable bowel syndrome (in adults), [and] first-degree relatives of people with celiac disease” (NICE, 2022).
“Any test is accurate only if a gluten-free containing diet is eaten during the diagnostic process and advise the person not to start a gluten-free diet until diagnosis is confirmed by a specialist, even if the results of a serological test are positive” (NICE,2022).
Further, serological testing for CD could be considered in patients with “metabolic bone disorder (reduced bone mineral density or osteomalacia), unexplained neurological symptoms (particularly peripheral neuropathy or ataxia), unexplained subfertility or miscarriage, persistently raised liver enzymes with unknown cause, dental enamel defects, Down’s syndrome, and Turner syndrome” (NICE, 2022).
Finally, regarding serological testing:
- “Test for total IgA and IgA tTG as the first choice.
- Use IgA EMA if IgA tTG is weakly positive.
- Consider using IgG EMA, IgG DGP or IgG tTG if IgA is deficient (IgA deficiency is defined as total IgA less than 0.07 g per litre) (NICE, 2022).”
In 2015, the National Institute for Health and Care Excellence (NICE) recommended CD serologic testing in symptomatic young people and adults with the following algorithm (NICE, 2015):
- First test for total serum IgA and TTG.
- Next test for IgA endomysial antibodies (EMA) if TTG is inconclusive (i.e., weakly positive).
- “Consider using IgG EMA, IgG deamidated gliadin peptide (DGP) or IgG tTG if IgA is deficient.”
For children with suspected CD, they recommend:
- First test for total serum IgA and TTG.
- “Consider using IgG EMA, IgG DGP or IgG tTG if IgA is deficient.”
NICE also recommends offer CD testing for people with any of the following:
- Autoimmune thyroid disease
- Persistent unexplained abdominal or gastrointestinal symptoms
- Irritable bowel syndrome
- Type 1 diabetes
- First-degree relatives (parents, siblings, or children) with coeliac disease
- Other symptoms indicative of possible CD, including faltering growth in children, prolonged fatigue, unexpected weight loss, severe or persistent mouth ulcers, unexplained dietary deficiencies
NICE also recommends considering CD testing for people with the following:
- Metabolic bone disorder
- Unexplained neurological symptoms
- Unexplained subfertility or recurrent miscarriage
- Down’s syndrome or Turner’s syndrome
- Dental enamel defects
- Persistent elevated hepatic enzymes of unknown etiology
They do note that “People who are following a normal diet (containing gluten) should be advised to eat gluten in more than 1 meal every day for at least 6 weeks before testing for coeliac disease (NICE, 2016).”
NICE indicates that HLA testing should not be done as part of the initial testing. Also, “Only consider using HLA DQ2 (DQ2.2 and DQ2.5)/DQ8 testing in the diagnosis of coeliac disease in specialist settings (for example, in children who are not having a biopsy, or in people who already have limited gluten ingestion and choose not to have a gluten challenge) (NICE, 2015).”
United States Preventive Services Task Force
The United States Preventative Services Task Force (Bibbins-Domingo et al., 2017) recently published guidelines on the screening of asymptomatic populations for celiac disease and found that:
“The USPSTF concludes that the current evidence is insufficient to assess the balance of benefits and harms of screening for celiac disease in asymptomatic persons. Evidence is lacking, and the balance of benefits and harms cannot be determined.” However, it was noted that: “Persons at increased risk for celiac disease include those who have a positive family history (e.g., a first- or second-degree relative), with an estimated prevalence of 5% to 20%, and persons with other autoimmune diseases (eg, type 1 diabetes mellitus, inflammatory luminal gastrointestinal disorders, Down syndrome, Turner syndrome, IgA deficiency, and IgA nephropathy). Several specialty societies recommend screening in these populations.”
World Gastroenterology Organisation (WGO) Global Guidelines
The WGO published guidelines on CD testing in 2017. A cascade with “resource-sensitive” options is listed.
The “Gold Standard” lists the following items for diagnosis of CD:
- Celiac disease–specific antibodies: assessment and intestinal biopsy
- Anti-tTG IgA or anti-EMA IgA, and total IgA to exclude IgA deficiency
- In case of selective IgA deficiency, IgG-based tests should be used: anti-DGP, anti-tTG, or EMA (the latter 2 are highly
- sensitive, but with lower specificity)
- Symptomatic patients with a positive serological test or a titer just below the cut-off (borderline) should be referred for endoscopy with multiple duodenal biopsies to confirm or exclude the diagnosis of celiac disease. Pitfalls in histologic diagnosis are common, and findings are characteristic, but not specific
- Asymptomatic patients with a positive serological test should be retested after consuming a gluten-containing diet for 3 months, to confirm persistent seropositivity before referral for endoscopy
The following items are listed for management of CD:
- Follow-up monitoring, including antibody tests (anti-tTG IgA or DGP-IgG in case of IgA deficiency): after 3 to 6 mo in the first year and once a year thereafter in stable patients responding to the gluten-free diet
The WGO also notes that although the presence of HLA risk alleles is “necessary” for celiac disease, it is insufficient for CD development. However, it does have a high negative predictive value, in that absence of those risk alleles excludes CD as a diagnosis.
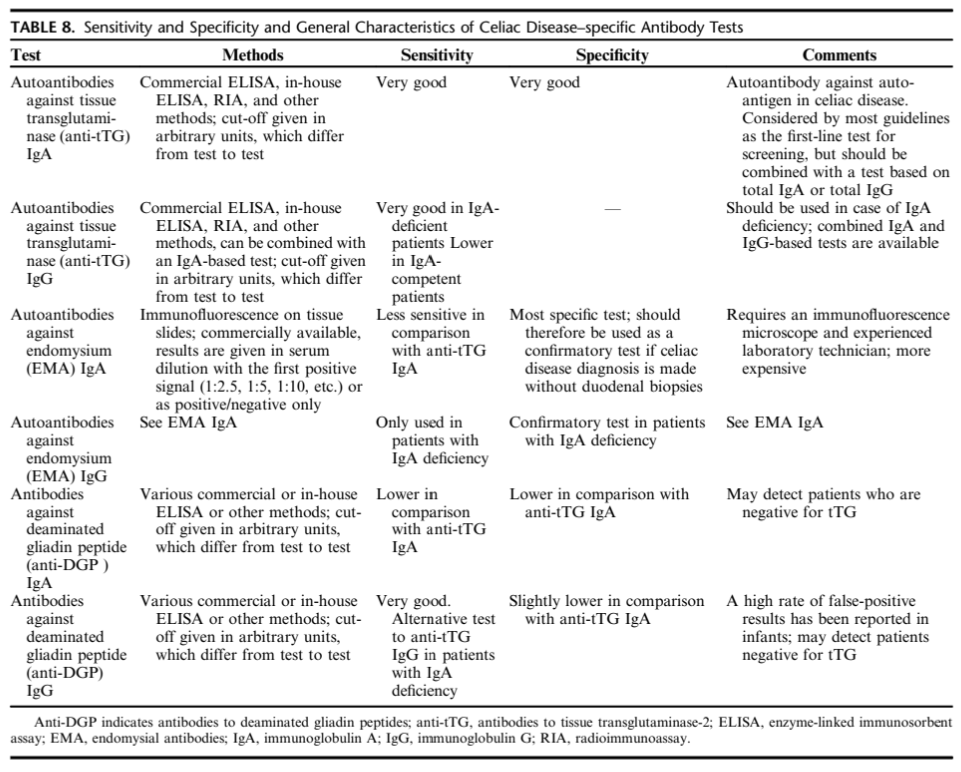
The WGO notes two main groups of serological markers for untreated CD:
- Autoantibodies targeting the auto-antigen: EMA and anti-tTG antibodies
- Antibodies targeting the offending agent (gliadin): anti- bodies against synthetic deamidated gliadin peptides (anti-DGPs)
A summary of the characteristics of CD antibody tests is listed below:
The WGO also lists several conditions associated with a higher risk of CD. Those conditions are as follows:
- Type 1 diabetes mellitus
- Autoimmune thyroid disease
- Autoimmune liver disease
- Down syndrome
- Turner syndrome
- Williams syndrome
- Selective IgA deficiency
- Unexplained elevated serum aminotransferase levels
The WGO also recommends that first-degree relatives of index (affected) patients to be screened for CD.
Finally, the WHO recommends against use of urine, stool, or saliva measurements in clinical practice, as they have a “lower performance” than blood-based tests (Bai & Ciacci, 2017).
European Society for the Study of Coeliac Disease (ESsCD)
The ESsCD published guidelines on CD, including recommendations on serological and genetic testing. These recommendations are listed below:
- “Adult patients with symptoms, signs or laboratory evidence suggestive of malabsorption should be tested with serology for CD. (Strong recommendation, high level of evidence)”
- “Screening of asymptomatic first-degree family member of CD patient is recommended. If available, HLA-typing may be offered as the first-line test; if negative, no further work-up is needed. (Conditional recommendation, high level of evidence)”
- “CD should be excluded in patients with unexplained elevation of serum aminotransferase levels. (Strong recommendation, high level of evidence)”
- “T1DM should be screened regularly for CD. (Strong recommendation, high level of evidence)”
- “IgA-TG2 antibody is the preferred single test for detection of CD at any age. (Strong recommendation, high level of evidence)”
- “Total IgA level needs to be measured concurrently with serology testing to determine whether IgA levels are sufficient. (Strong recommendation, moderate level of evidence)”
- “In patients with selective total IgA-deficiency, IgG-based testing (IgG-DGPs or IgG-TG2) should be performed at diagnosis and follow-up. (Strong recommendation, moderate level of evidence)”
- “All diagnostic serologic testing should be done while patients on a gluten-containing diet. (Strong recommendation, high level of evidence)”
- “Antibodies directed against native gliadin (AGA) are not recommended for the primary detection of CD. (Strong recommendation, high level of evidence)”
- “Intestinal-permeability tests are neither sensitive nor specific and are not recommended for CD diagnosis. (Strong recommendation, moderate level of evidence)”
- “Serum I-FABP might be useful in identifying dietary non-adherence and unintentional gluten intake. (Strong recommendation, moderate level of evidence)”
- “A newly diagnosed adult CD patient should undergo testing to uncover deficiencies of essential micronutrient, e.g., iron, folic acid, vitamin D and vitamin B12. (Strong recommendation, moderate level of evidence)”
- “CD diagnosis may be made without duodenal biopsy in symptomatic children with high TG2 levels (> 10 times ULN) and EMA in the presence of HLA-DQ2/8. The diagnosis is confirmed by an antibody decline and preferably a clinical response to a GFD”. (Conditional recommendation, moderate level of evidence)
The ESsCD also lists recommendations for HLA-DQ2/8 typing, which are as follows:
- “A negative HLA test is helpful to exclude the possibility of CD. This is especially helpful in those already on a GFD before testing.”
- “When diagnosis of CD is uncertain, e.g., negative serology, but histology suggestive of CD.”
- “To distinguish siblings who can be reassured that it is unlikely that they will develop CD from those who need to be monitored. Furthermore, the data on the quality of life on a GFD in those patients detected by screening are conflicting, but there is a trend towards improvement. Also, the lack of understanding of the natural history of undiagnosed CD may justify screening asymptomatic persons.”
- “In subjects with other autoimmune diseases and some genetic disorders who should be investigated for CD.”
- “HLA-DQ2/DQ8 testing should not be used routinely in the initial diagnosis of CD. It is recommended that the results of such testing should be included along with a caution that patients at risk should be serologically tested for CD without changing their diet. (Strong recommendation, moderate level of evidence) (Al-Toma et al., 2019).”
British Society of Gastroenterology (BSG)
In 2014 the BSG published guidelines for the diagnosis and management of adult CD. The following guidelines were included:
- “Diagnosis of CD requires duodenal biopsy when the patient is on a gluten-containing diet and for the vast majority of adult patients also positive serology. (Grade B)
- Biopsy remains essential for the diagnosis of adult CD and cannot be replaced by serology. Follow-up should aim at strict adherence to a gluten-free diet. (Grade B)
- In individuals undergoing an upper endoscopy in whom laboratory tests or symptoms or endoscopic features suggest CD, duodenal biopsy should be considered. (Grade C)
- HLA typing should be used to rule out CD. A positive DQ2.5 or DQ8 can never confirm the diagnosis. (Grade B)
- HLA typing should be used in individuals who are self-treated on a GFD and never had appropriate testing for CD before changing their diet. (Grade B)
- HLA typing can be used to rule out CD, and minimise future testing, in high-risk individuals with CD, for example, first-degree relatives. (Grade B)
- The diagnosis of CD requires duodenal biopsy when the patient is on a gluten-containing diet and for the vast majority of adult patients also positive serology. (Grade B)
- Duodenal biopsy should be retained as the mainstay for the diagnosis of adult CD and cannot be replaced by serology. (Grade B)
- At endoscopy, if there is suspicion of CD, then at least four biopsy specimens should be obtained, including a duodenal bulb biopsy. (Grade C)
- In serologically negative patients showing signs of malabsorption (such as anaemia or diarrhoea) or a family history of CD, a duodenal biopsy should be considered. (Grade C)
- Follow-up biopsies may be considered in patients with CD, and are potentially helpful in identifying patients at increased risk of lymphoma. (Grade B) (Ludvigsson et al., 2014)”
British Society of Paediatric Gastroenterology, Hepatology, and Nutrition (BSPGHAN) and Coeliac UK
In 2013, the BSPGHAN and Coeliac UK published joint guidelines for the management of CD in children. These guidelines note that “Anti-tTG antibody positivity alone is insufficient for diagnosis. Therapeutic trials of GFD are NOT indicated if CD is suspected.” Further, if the patient is symptomatic, IgA and IgA tTG should be checked first. “
- “If tTG negative and IgA normal, CD unlikely: If IgA low, then further testing (e.g., IgG tTG and possible biopsy) is required.
- If tTG raised — but less than 10× upper limit of normal for assay: Duodenal biopsy is required. At endoscopy, take four biopsies from D2 or lower and 1 – 2 from duodenal bulb (as patchy changes may be present). Ensure adequate gluten intake prior to testing with advice from dietician if necessary
- If tTG raised — and greater than 10× upper limit of normal for assay: Take further blood sample to check IgA-EMA and determine HLA-DQ2/HLA-DQ8 typing. If EMA+ and patient either DQ2 or DQ8, the diagnosis is confirmed without the need for a duodenal biopsy. If EMA antibody testing is not locally available, a second strongly positive tTG antibody may be substituted and serum saved for later EMA testing (Murch et al., 2013).”
North American Society for the Study of Celiac Disease (NASSCD)
In 2017, the NASSCD uploaded a guideline for celiac disease diagnosis in adults, along with a diagram detailing the algorithm for a positive celiac disease diagnosis with presenting GI and/or extraintestinal symptoms and signs. They state:
“Celiac disease (CD) may be suspected in
- Symptomatic patients with
- Gastrointestinal symptoms/signs: diarrhea, weight loss, gas/bloating, constipation (more commonly in children), hypertransaminasemia
- Extraintestinal symptoms/signs: iron deficiency anemia, dermatitis herpetiformis, osteoporosis and neuropsychiatric conditions, such as neuropathy or ataxia
- Patients with associated conditions
- Type 1 diabetes mellitus
- Autoimmune thyroiditis
- Other autoimmune conditions
- Down syndrome
- First-degree family members of celiac patients”
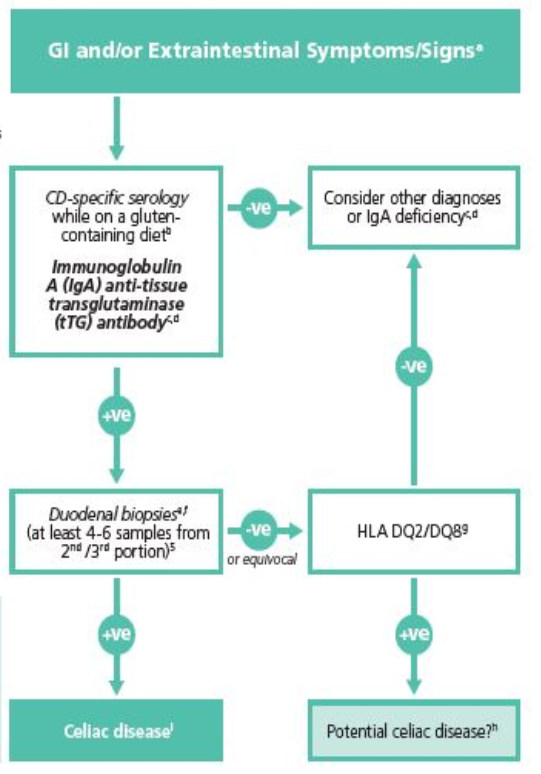
(+ve indicates positive, -ve indicates negative)
The NASSCD has also included the following comments with regards to its algorithm and suspicion of CD:
- “Screening for celiac disease in high-risk asymptomatic populations is controversial due to unknown natural history and potential benefits.
- If patient self-started a gluten-free diet, consider testing after challenge with > 3 g of gluten per day (equivalent to 1 – 2 slices of bread per day) for at least two weeks.
- The addition of total IgA is useful to detect IgA deficiency.
- An alternative approach is to include both IgA and IgG-based testing, such as IgG-deamidated gliadin peptides (DGPs).
- There is scarce data using serology alone for diagnosis of CD. Combined use of biopsy and serologic analyses for diagnosis of celiac disease is recommended in adults.
- Current guidelines recommend 1 – 2 biopsies from the bulb in addition to at least 4 biopsies from distal duodenum. However, the advantages, (increased sensitivity) and disadvantages (reduced specificity) of bulb biopsies are under scrutiny.
- HLA DQ2/DQ8 negative excludes CD in majority of cases.
- Other reasons for discrepant serology and biopsies include reduced gluten in the diet, inadequate biopsy sampling, and lack of expert histopathology reporting.
- Celiac disease diagnosis is confirmed after clinical and/or histology improvement after gluten-free diet” (NASSCD, 2017).
American Academy of Family Physicians (AAFP)
In January 2014, the AAFP released a set of recommendations regarding the diagnosis and management of celiac disease. Based on “consensus, disease-oriented evidence, usual practice, expert opinion, or case series (Evidence Rating: C),” the AAFP stated the following:
- “Immunoglobulin A tissue transglutaminase should be used as the first-line test for serologic diagnosis of suspected celiac disease.
- Small bowel biopsy should be used to confirm the diagnosis of celiac disease in most patients” (Pelkowski & Viera, 2014).
Table of Terminology
|
Term |
Definition |
|
AAFP |
American Academy of Family Physicians |
|
ACG |
American College of Gastroenterology |
|
AGA |
American Gastroenterological Association |
|
ANG |
Anti-native gliadin antibodies |
|
BSG |
British Society of Gastroenterology |
|
BSPGHAN |
British Society of Pediatric Gastroenterology, Hepatology, and Nutrition |
|
CD |
Celiac disease |
|
CMS |
Centers for Medicare & Medicaid Services |
|
DGP |
Deamidated gliadin peptides |
|
DTC |
Direct to consumer |
|
ELISA |
Enzyme-linked immunosorbent assay |
|
EMA |
Endomysial antibodies |
|
ESP-GHAN |
European Society of Pediatrics Gastroenterology, Hepatology, and Nutrition |
|
ESsCD |
European Society for the Study of Coeliac Disease |
|
GFD |
Gluten-free diet |
|
HLA |
Human leukocyte antigen |
|
HLA-DQA1 |
Major histocompatibility complex, class II, DQ alpha 1 gene |
|
HLA-DQB1 |
Major histocompatibility complex, class II, DQ beta 1 gene |
|
IgA |
Immunoglobulin A |
|
LDTs |
Laboratory-developed tests |
|
NASPGHAN |
North American Society of Pediatric Gastroenterology, Hepatology, and Nutrition |
|
NASSCD |
North American Society for the Study of Celiac Disease |
|
NCGS |
Non-celiac gluten sensitivity |
|
NICE |
National Institute for Health and Care Excellence |
|
NIDDK |
National Institute of Diabetes ad Digestive and Kidney Diseases |
|
SIgE |
Specific immunoglobulin-E |
|
SSOP |
Sequence-specific oligonucleotide probe |
|
TIDM |
Type 1 diabetes mellitus |
|
TTG |
Tissue transglutaminase |
|
ULN |
Upper limit of normal |
|
USPSTF |
United State Preventive Services Task Force |
|
WA |
Wheat allergy |
|
WGO |
World Gastroenterology Organization |
|
ZED1227 |
Oral transgluaminase 2 inhibitor |
References:
- Al-Toma, A., Volta, U., Auricchio, R., Castillejo, G., Sanders, D. S., Cellier, C., Mulder, C. J., & Lundin, K. E. A. (2019). European Society for the Study of Coeliac Disease (ESsCD) guideline for coeliac disease and other gluten-related disorders. United European Gastroenterol J, 7(5), 583-613. https://doi.org/10.1177/2050640619844125
- Arenda. (2020). SIMTOMAX DGP TEST. https://www.arenda.hr/en/simtomax-dgp-test.aspx
- Bai, J. C., & Ciacci, C. (2017). World Gastroenterology Organisation Global Guidelines: Celiac Disease February 2017. J Clin Gastroenterol, 51(9), 755-768. https://doi.org/10.1097/mcg.0000000000000919
- Bajor, J., Szakács, Z., Farkas, N., Hegyi, P., Illés, A., Solymár, M., Pétervári, E., Balaskó, M., Pár, G., Sarlós, P., Szűcs, Á., Czimmer, J., Szemes, K., Huszár, O., Varjú, P., & Vincze, Á. (2019). Classical celiac disease is more frequent with a double dose of HLA-DQB1*02: A systematic review with meta-analysis. PLoS One, 14(2), e0212329. https://doi.org/10.1371/journal.pone.0212329
- Bibbins-Domingo, K., Grossman, D. C., Curry, S. J., Barry, M. J., Davidson, K. W., Doubeni, C. A., Ebell, M., Epling, J. W., Jr., Herzstein, J., Kemper, A. R., Krist, A. H., Kurth, A. E., Landefeld, C. S., Mangione, C. M., Phipps, M. G., Silverstein, M., Simon, M. A., & Tseng, C. W. (2017). Screening for Celiac Disease: US Preventive Services Task Force Recommendation Statement. Jama, 317(12), 1252-1257. https://doi.org/10.1001/jama.2017.1462
- Brown, N. K., Guandalini, S., Semrad, C., & Kupfer, S. S. (2019). A Clinician's Guide to Celiac Disease HLA Genetics. Am J Gastroenterol, 114(10), 1587-1592. https://doi.org/10.14309/ajg.0000000000000310
- Bufler, P., Heilig, G., Ossiander, G., Freudenberg, F., Grote, V., & Koletzko, S. (2015). Diagnostic performance of three serologic tests in childhood celiac disease. Z Gastroenterol, 53(2), 108-114. https://doi.org/10.1055/s-0034-1385704
- Caio, G., Volta, U., Sapone, A., Leffler, D. A., De Giorgio, R., Catassi, C., & Fasano, A. (2019). Celiac disease: a comprehensive current review. BMC Med, 17(1), 142. https://doi.org/10.1186/s12916-019-1380-z
- CDF. (2018). What is Celiac disease? Celiac Disease Foundation. Retrieved 08/23/2018 from https://celiac.org/celiac-disease/understanding-celiac-disease-2/what-is-celiac-disease/
- FDA. (2014). IG_PLEX CELIAC DGP PANEL. https://www.accessdata.fda.gov/scripts/cdrh/devicesatfda/index.cfm?db=pmn&id=K140691
- FDA. (2017). DECISION SUMMARY. https://www.accessdata.fda.gov/cdrh_docs/reviews/DEN160026.pdf
- FDA. (2021, June 16). Aptiva Celiac Disease IgA Reagent. https://www.accessdata.fda.gov/cdrh_docs/reviews/K193604.pdf
- Gould, M. J., Mahmud, F. H., Clarke, A. B. M., McDonald, C., Saibil, F., Punthakee, Z., & Marcon, M. A. (2021). Accuracy of Screening Tests for Celiac Disease in Asymptomatic Patients With Type 1 Diabetes. Am J Gastroenterol, 116(7), 1545-1549. https://doi.org/10.14309/ajg.0000000000001193
- Hill, I. D., Fasano, A., Guandalini, S., Hoffenberg, E., Levy, J., Reilly, N., & Verma, R. (2016). NASPGHAN Clinical Report on the Diagnosis and Treatment of Gluten-related Disorders. J Pediatr Gastroenterol Nutr, 63(1), 156-165. https://doi.org/10.1097/mpg.0000000000001216
- Husby, S., Koletzko, S., Korponay-Szabó, I., Kurppa, K., Mearin, M. L., Ribes-Koninckx, C., Shamir, R., Troncone, R., Auricchio, R., Castillejo, G., Christensen, R., Dolinsek, J., Gillett, P., Hróbjartsson, A., Koltai, T., Maki, M., Nielsen, S. M., Popp, A., Størdal, K., . . . Wessels, M. (2020). European Society Paediatric Gastroenterology, Hepatology and Nutrition Guidelines for Diagnosing Coeliac Disease 2020. J Pediatr Gastroenterol Nutr, 70(1), 141-156. https://doi.org/10.1097/mpg.0000000000002497
- Husby, S., Koletzko, S., Korponay-Szabó, I. R., Mearin, M. L., Phillips, A., Shamir, R., Troncone, R., Giersiepen, K., Branski, D., Catassi, C., Lelgeman, M., Mäki, M., Ribes-Koninckx, C., Ventura, A., Zimmer, K. P., & for the ESPGHAN Working Group on Coeliac Disease Diagnosis, o. b. o. t. E. G. C. (2012). European Society for Pediatric Gastroenterology, Hepatology, and Nutrition Guidelines for the Diagnosis of Coeliac Disease. Journal of Pediatric Gastroenterology and Nutrition, 54(1), 136-160. https://doi.org/10.1097/MPG.0b013e31821a23d0
- Husby, S., Murray, J. A., & Katzka, D. A. (2019). AGA Clinical Practice Update on Diagnosis and Monitoring of Celiac Disease - Changing Utility of Serology and Histologic Measures: Expert Review. Gastroenterology, 156(4), 885-889. https://doi.org/10.1053/j.gastro.2018.12.010
- Jansson-Knodell, C. L., Hujoel, I. A., West, C. P., Taneja, V., Prokop, L. J., Rubio-Tapia, A., & Murray, J. A. (2019). Sex Difference in Celiac Disease in Undiagnosed Populations: A Systematic Review and Meta-analysis. Clin Gastroenterol Hepatol, 17(10), 1954-1968.e1913. https://doi.org/10.1016/j.cgh.2018.11.013
- Kelly, C. P. (2022, April 7). Diagnosis of celiac disease in adults. https://www.uptodate.com/contents/diagnosis-of-celiac-disease-in-adults
- Ludvigsson, J. F., Bai, J. C., Biagi, F., Card, T. R., Ciacci, C., Ciclitira, P. J., Green, P. H., Hadjivassiliou, M., Holdoway, A., van Heel, D. A., Kaukinen, K., Leffler, D. A., Leonard, J. N., Lundin, K. E., McGough, N., Davidson, M., Murray, J. A., Swift, G. L., Walker, M. M., . . . Sanders, D. S. (2014). Diagnosis and management of adult coeliac disease: guidelines from the British Society of Gastroenterology. Gut, 63(8), 1210-1228. https://doi.org/10.1136/gutjnl-2013-306578
- Mubarak, A., Spierings, E., Wolters, V., van Hoogstraten, I., Kneepkens, C. M., & Houwen, R. (2013). Human leukocyte antigen DQ2.2 and celiac disease. J Pediatr Gastroenterol Nutr, 56(4), 428-430. https://doi.org/10.1097/MPG.0b013e31827913f9
- Murch, S., Jenkins, H., Auth, M., Bremner, R., Butt, A., France, S., Furman, M., Gillett, P., Kiparissi, F., Lawson, M., McLain, B., Morris, M. A., Sleet, S., & Thorpe, M. (2013). Joint BSPGHAN and Coeliac UK guidelines for the diagnosis and management of coeliac disease in children. Arch Dis Child, 98(10), 806-811. https://doi.org/10.1136/archdischild-2013-303996
- NASSCD. (2017, October). Adult Guideline - Celiac Disease Diagnosis. https://www.theceliacsociety.org/cd-adult_diagnosis_guide
- Nellikkal, S. S., Hafed, Y., Larson, J. J., Murray, J. A., & Absah, I. (2019). High Prevalence of Celiac Disease Among Screened First-Degree Relatives. Mayo Clin Proc, 94(9), 1807-1813. https://doi.org/10.1016/j.mayocp.2019.03.027
- NICE. (2015, 09/02/2015). Coeliac disease: recognition, assessment and management. National Institute for Health and Care Excellence. Retrieved 08/23/2018 from https://www.nice.org.uk/guidance/ng20/resources/coeliac-disease-recognition-assessment-and-management-pdf-1837325178565
- NICE. (2016, 10/19/2016). Coeliac disease. National Institute for Health and Care Excellence. Retrieved 08/23/2018 from https://www.nice.org.uk/guidance/qs134/resources/coeliac-disease-pdf-75545419042501
- NICE. (2022). Coeliac disease overview. https://pathways.nice.org.uk/pathways/coeliac-disease
- NIDDK. (2016, 06/2016). Symptoms & Causes of Celiac Disease. U.S. Department of Health and Human Services. Retrieved 09/08/2020 from https://www.niddk.nih.gov/health-information/digestive-diseases/celiac-disease/symptoms-causes
- NIDDK. (2020, October). Definition & Facts for Celiac Disease. National Institute of Diabetes and Digestive and Kidney Diseases. Retrieved 07/11/2021 from https://www.niddk.nih.gov/health-information/digestive-diseases/celiac-disease/definition-facts
- Olen, O., Gudjonsdottir, A. H., Browaldh, L., Hessami, M., Elvin, K., Liedberg, A. S., Neovius, M., & Grahnquist, L. (2012). Antibodies against deamidated gliadin peptides and tissue transglutaminase for diagnosis of pediatric celiac disease. J Pediatr Gastroenterol Nutr, 55(6), 695-700. https://doi.org/10.1097/MPG.0b013e3182645c54
- Paul, S. P., Hoghton, M., & Sandhu, B. (2017). Limited role of HLA DQ2/8 genotyping in diagnosing coeliac disease. Scott Med J, 62(1), 25-27. https://doi.org/10.1177/0036933016689008
- Pelkowski, T. D., & Viera, A. J. (2014). Celiac disease: diagnosis and management. Am Fam Physician, 89(2), 99-105.
- Profaizer, T., Pole, A., Monds, C., Delgado, J. C., & Lázár-Molnár, E. (2020). Clinical utility of next generation sequencing based HLA typing for disease association and pharmacogenetic testing. Hum Immunol, 81(7), 354-360. https://doi.org/10.1016/j.humimm.2020.05.001
- Rubio-Tapia, A., Hill, I. D., Kelly, C. P., Calderwood, A. H., & Murray, J. A. (2013). ACG clinical guidelines: diagnosis and management of celiac disease. Am J Gastroenterol, 108(5), 656-676; quiz 677. https://doi.org/10.1038/ajg.2013.79
- Sakly, W., Mankai, A., Ghdess, A., Achour, A., Thabet, Y., & Ghedira, I. (2012). Performance of anti-deamidated gliadin peptides antibodies in celiac disease diagnosis. Clin Res Hepatol Gastroenterol, 36(6), 598-603. https://doi.org/10.1016/j.clinre.2012.01.008
- Sarna, V. K., Lundin, K. E. A., Morkrid, L., Qiao, S. W., Sollid, L. M., & Christophersen, A. (2018). HLA-DQ-Gluten Tetramer Blood Test Accurately Identifies Patients With and Without Celiac Disease in Absence of Gluten Consumption. Gastroenterology, 154(4), 886-896.e886. https://doi.org/10.1053/j.gastro.2017.11.006
- Selleski, N., Almeida, L. M., Almeida, F. C., Pratesi, C. B., Nobrega, Y. K. M., & Gandolfi, L. (2018). PREVALENCE OF CELIAC DISEASE PREDISPOSING GENOTYPES, INCLUDING HLA-DQ2.2 VARIANT, IN BRAZILIAN CHILDREN. Arq Gastroenterol, 55(1), 82-85. https://doi.org/10.1590/s0004-2803.201800000-16
- Silvester, J. A., Kurada, S., Szwajcer, A., Kelly, C. P., Leffler, D. A., & Duerksen, D. R. (2017). Tests for Serum Transglutaminase and Endomysial Antibodies Do Not Detect Most Patients With Celiac Disease and Persistent Villous Atrophy on Gluten-free Diets: a Meta-analysis. Gastroenterology, 153(3), 689-701.e681. https://doi.org/10.1053/j.gastro.2017.05.015
- Stankovic, B., Radlovic, N., Lekovic, Z., Ristic, D., Radlovic, V., Nikcevic, G., Kotur, N., Vucicevic, K., Kostic, T., Pavlovic, S., & Zukic, B. (2014). HLA genotyping in pediatric celiac disease patients. Bosn J Basic Med Sci, 14(3), 171-176. https://doi.org/10.17305/bjbms.2014.3.28
- Tangermann, P., Branchi, F., Itzlinger, A., Aschenbeck, J., Schubert, S., Maul, J., Liceni, T., Schröder, A., Heller, F., Spitz, W., Möhler, U., Graefe, U., Radke, M., Trenkel, S., Schmitt, M., Loddenkemper, C., Preiß, J. C., Ullrich, R., Daum, S., . . . Schumann, M. (2019). Low Sensitivity of Simtomax Point of Care Test in Detection of Celiac Disease in a Prospective Multicenter Study. Clin Gastroenterol Hepatol, 17(9), 1780-1787.e1785. https://doi.org/10.1016/j.cgh.2018.09.032
- Tye-Din, J. A., Galipeau, H. J., & Agardh, D. (2018). Celiac Disease: A Review of Current Concepts in Pathogenesis, Prevention, and Novel Therapies. Front Pediatr, 6, 350. https://doi.org/10.3389/fped.2018.00350
- Vijzelaar, R., van der Zwan, E., van Gammeren, A., Yilmaz, R., Verheul, A., van Hoogstraten, I., de Baar, E., Schrauwen, L., & Kortlandt, W. (2016). Rapid Detection of the Three Celiac Disease Risk Genotypes HLA-DQ2.2, HLA-DQ2.5, and HLA-DQ8 by Multiplex Ligation-Dependent Probe Amplification. Genet Test Mol Biomarkers, 20(3), 158-161. https://doi.org/10.1089/gtmb.2015.0233
Coding Section
|
Code |
Number |
Description |
|
CPT |
81376 |
HLA Class II typing, low resolution (e.g., antigen equivalents); one locus (e.g., HLA-DRB1, -DRB3/4/5, -DQB1, -DQA1, -DPB1, or -DPA1), each |
|
|
81377 |
HLA Class II typing, low resolution (e.g., antigen equivalents); one antigen equivalent, each |
|
|
81382 |
HLA Class II typing, high resolution (i.e., alleles or allele groups); one locus (e.g., HLA-DRB1, -DRB3/4/5, -DQB1, -DQA1, -DPB1, or -DPA1), each |
|
|
81383 |
HLA Class I typing, high resolution (i.e., alleles or allele groups); one allele or allele group (e.g., HLA-DBQ1*06:02P), each |
|
|
82784 |
Gammaglobulin (immunoglobulin); IgA, IgD, IgG, IgM, each |
|
|
83516 |
Immunoassay for analyte other than infectious agent antibody or infectious agent antigen; qualitative or semiquantitative, multiple method |
|
|
86231 (effective 01/01/2022) |
Endomysial antibody (EMA), each immunoglobulin (Ig) class |
|
|
86255 |
Fluorescent noninfectious agent anitbody, screen, each antibody |
|
|
86256 |
Titer, each antibody (fluorescent technique for antigen identification in tissue, use 88346, for indirect fluorescence, use 88347) (FTA, use 86780) (Gel [agar] diffusion tests, use 86331) |
|
|
86258 (effective 01/01/2022) |
Gliadin (deamidated) (DGP) antibody, each immunoglobulin (Ig) class |
|
|
86364 (effective 01/01/2022) |
Tissue transglutaminase, each immunoglobulin (Ig) class |
|
|
88305 |
Level IV - Surgical pathology, gross and microscopic examination, colon biopsy |
|
ICD-10-CM (effective 10/01/15) |
K90.0 |
Celiac disease |
|
|
E30.0 |
Delayed puberty |
|
|
E53.8 |
Deficiency of other specified B group vitamins |
|
|
E53.9 |
Vitamin B deficiency, unspecified |
|
|
E10.10-E10.9 |
Type 1 diabetes mellitus |
|
|
M80.00XA-M80.88XS |
Age-related osteoporosis with current pathological fracture, unspecified site |
|
|
M81.6 |
Localized osteoporosis (Lequesne) |
|
|
M81.8 |
Other osteoporosis without current pathological fracture |
|
|
M83.0-M83.9 |
Adult osteomalacia |
|
|
N91.0-N91.2 |
Absent, scanty and rare menstruation |
|
|
O03.0-O03.9 |
Spontaneous abortion |
|
|
Q96.0-Q96.9 |
Turner's syndrome |
|
|
Q93.82 |
Williams syndrome |
|
|
R62.7 |
Adult failure to thrive |
|
|
R62.51 |
Failure to thrive (child) |
|
|
R62.52 |
Short stature (child) |
|
|
R11.0-R11.9 |
Nausea and vomiting |
|
ICD-10-PCS (effective 10/01/15) |
|
Not applicable. ICD-10-PCS codes are only used for inpatient services. There are no ICD procedure codes for laboratory tests. |
Procedure and diagnosis codes on Medical Policy documents are included only as a general reference tool for each policy. They may not be all-inclusive.
This medical policy was developed through consideration of peer-reviewed medical literature generally recognized by the relevant medical community, U.S. FDA approval status, nationally accepted standards of medical practice and accepted standards of medical practice in this community, Blue Cross Blue Shield Association technology assessment program (TEC) and other nonaffiliated technology evaluation centers, reference to federal regulations, other plan medical policies, and accredited national guidelines.
"Current Procedural Terminology © American Medical Association. All Rights Reserved"
History From 2014 Forward
| 11/08/2022 | Annual review, no change to policy intent. Policy reformatted for clarity. Adding table of terminology. Updating rationale, references and coding. |
|
12/8/2021 |
Updating policy with 2022 coding. Adding code 86231, 86258 and 86364. No other change made. |
|
10/01/2021 |
Annual review, no change to policy intent. Updating background, regulatory status, rationale, references and policy number. |
|
10/01/2020 |
Annual review, reformatting policy and adding "note 1" for clarity. Updating coding, description, rationale and references. |
|
10/17/2019 |
Annual review, no change to policy intent. Reformatting for clarity, updating coding. |
|
11/05/2018 |
Annual review, adding HLA-DQ- gluten testing as investigational, also adding rapid antigen point of care testing for anti-TTG as not medically necessary. Adding panel testing, multiples or multi analyte testing as not medically necessary. No other changes. |
|
11/02/2017 |
Annual review, updating medical necessity criteria for more specificity regarding symptoms suggestive of celiac disease. No change to policy |
|
04/26/2017 |
Updated category to Laboratory. No other changes. |
|
04/05/2017 |
Annual review, no change to policy intent. |
|
06/13/2016 |
Corrected a typo error in the policy section. |
|
05/09/2016 |
Interim review adding criteria in policy section. |
|
04/07/2015 |
Annual review, no change to policy intent. Adding coding. |
|
04/10/2014 |
Annual review. Adding related policies and benefit application. Updated guidelines. No change to policy intent. |