
Fibromyalgia Testing - CAM 272
Description
Fibromyalgia (FM) is a chronic diffuse pain condition and the most common cause of chronic widespread musculoskeletal pain (Goldenberg, 2022a). It is also known by “diffuse myofascial pain syndrome,” “fibromyalgia-fibromyositis syndrome,” or “fibromyalgia syndrome” (Ada, 2020). FM has The etiology and pathophysiology of FM is generally unknown, but it can be found with “fatigue, cognitive disturbance psychiatric symptoms, and multiple somatic symptoms;” however, presentation may vary from patient to patient (Goldenberg, 2022a; Kimura & Walco, 2022). Controversy has arisen regarding the disease origin, as it has been considered to be psychogenic or psychosomatic, but recent research indicates it as a disorder of pain regulation, a form of “central sensitization” (Goldenberg, 2022a).
Terms such as male and female are used when necessary to refer to sex assigned at birth.
Regulatory Status
A search for “Fibromyalgia” on 01/07/2021 yielded 0 lab testing results. A search for any specific tests of the genes likely implicated in FM also did not yield any lab testing results. Additionally, many labs have developed specific tests that they must validate and perform in house. These laboratory-developed tests (LDTs) are regulated by the Centers for Medicare & Medicaid (CMS) as high-complexity tests under the Clinical Laboratory Improvement Amendments of 1988 (CLIA ’88). As an LDT, the U. S. Food and Drug Administration has not approved or cleared this test; however, FDA clearance or approval is not currently required for clinical use (FDA, 2018).
Policy
Application of coverage criteria is dependent upon an individual’s benefit coverage at the time of the request.
The following does not meet coverage criteria due to a lack of available published scientific literature confirming that the test(s) is/are required and beneficial for the diagnosis and treatment of a patient’s illness.
- For the diagnosis of fibromyalgia or chronic pain syndromes, the following tests is considered NOT MEDICALLY NECESSARY:
- Genetic testing (e.g., mutation analysis, copy number variants, epigenetic analysis, mRNA expression, miRNA expression)
- Biomarker panel testing with proprietary algorithms and/or index scores (e.g., FM/a®, NutrEval FMV®).
Table of Terminology
|
Term |
Definition |
|
5HT |
Serotonin |
|
5-HT2A |
Serotonin 2A |
|
A1AT |
Alpha-1 antitrypsin |
|
AAPT |
ACTTION-APS Pain Taxonomy |
|
ACE I/D |
Angiotensin-converting enzyme I/D polymorphism |
|
ACR |
American College of Rheumatology |
|
ACTTION |
Analgesic, Anesthetic, and Addiction Clinical Trial Translations Innovations Opportunities and Networks |
|
ADRA1A |
Adrenoreceptor alpha 1A gene |
|
ADRB2 |
Adrenoreceptor beta 2 gene |
|
ADRB3 |
Adrenoreceptor beta 3 gene |
|
AMPA |
α-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid |
|
ANA/ENA |
Antinuclear antibody/extractable nuclear antigen antibody |
|
ANS |
Autonomic nervous system |
|
APS |
American Pain Society |
|
BDNF |
Brain derived neurotrophic factor gene |
|
CB-1 |
Cannabinoid receptor type 1 |
|
CLIA ’88 |
Clinical Laboratory Improvement Amendments Of 1988 |
|
CMS |
Centers for Medicare & Medicaid Services |
|
CNR1 |
Cannabinoid receptor 1 gene |
|
CNS |
Central nervous system |
|
CNV |
Copy number variant |
|
COMT |
Catecholamine o-methyl transferase gene |
|
CRA |
Canadian Rheumatology Association |
|
CRP |
C-reactive protein |
|
CSF |
Cerebrospinal fluid |
|
CWP |
Chronic widespread pain |
|
DNA |
Deoxyribonucleic acid |
|
DRD3 |
Dopamine receptor D3 gene |
|
EDN1 |
Endothelin 1 gene |
|
ESR |
Erythrocyte sedimentation rate |
|
FDA |
Food and Drug Administration |
|
FIQ |
Fibromyalgia-Impact Questionnaire |
|
FM |
Fibromyalgia |
|
GABRB3 |
Gamma-aminobutyric acid receptor subunit beta-3 gene |
|
GBP1 |
Guanylate binding protein 1 gene |
|
GCH1 |
Guanosine triphosphate (GTP) cyclohydrolase 1 gene |
|
GERD |
Gastroesophageal reflux disease |
|
GRIA4 |
Glutamate ionotropic receptor AMPA type subunit 4 gene |
|
HLA-DRB1 |
Human leukocyte antigen DR beta 1 gene |
|
HTR2A |
5-Hydroxytryptamine Receptor 2A gene |
|
HTR3A |
5-Hydroxytryptamine Receptor 3A gene |
|
HTR3B |
5-Hydroxytryptamine Receptor 3B gene |
|
IBS |
Irritable bowel syndrome |
|
IFN-γ |
Interferon-γ |
|
IGHV1OR21-1 |
Immunoglobulin domain-containing like protein |
|
IGLV3-25 |
Immunoglobulin lambda variable 3-25 |
|
IL-10 |
Interleukin-10 |
|
IL1RAP |
Interleukin-1 receptor accessor protein |
|
IL-4 |
Interleukin-4 gene |
|
IL-5 |
Interleukin-5 |
|
IL-6 |
Interleukin-6 |
|
IL-8 |
Interleukin-8 |
|
LDTs |
Laboratory-developed tests |
|
MAOA |
Monoamine oxidase A gene |
|
MAPK |
Mitogen-activated protein kinase |
|
MCP-1 |
Monocyte chemoattractant protein-1 |
|
MEFV |
Mediterranean fever gene |
|
METTL18 |
Methyltransferase-like 18 |
|
MIP-1β |
Macrophage inflammatory protein-1β |
|
MSP |
Multisite pain |
|
MTHFR |
Methylenetetrahydrofolate reductase gene |
|
MYT1L |
Myelin transcription factor 1 like gene |
|
NA |
Noradrenaline |
|
NRXN3 |
Neurexin 3 gene |
|
OPRM1 |
Opioid receptor mu 1 gene |
|
PBMC |
Plasma and peripheral blood mononuclear cells |
|
PHA |
Phytohemagglutinin |
|
PMA |
Phorbol-12-myristate-13-acetate |
|
RA |
Rheumatoid arthritis |
|
RGS4 |
Regulator of G protein signaling 4 gene |
|
SCL-90 |
Symptom Checklist-90 for Psychopathological Disorders |
|
SCN9A |
Sodium voltage-gated channel alpha subunit 9 gene |
|
SLC64A4 |
Solute carrier family 64 member 4 gene |
|
SERPINA1 |
Serpin family A member 1 gene |
|
SLE |
Systemic lupus erythematosus |
|
SNPs |
Single nucleotide polymorphisms |
|
SS |
Sjögren syndrome |
|
SS |
Symptom severity |
|
TAAR1 |
Trace amine-associated receptor 1 gene |
|
TACR1 |
Tachykinin receptor 1 gene |
|
TMD |
Temporomandibular joint disorder |
|
TPC |
Tender point count |
|
TPQ |
Tridimensional Personality Questionnaire |
|
TRPV2 |
Transient receptor potential vanilloid channel 2 gene |
|
TRPV3 |
Transient receptor potential vanilloid channel 3 gene |
|
TSH |
Thyroid stimulating hormone |
|
TSPO |
Translocator protein gene |
|
WPI |
Widespread pain index |
Rationale
Fibromyalgia (FM) is a condition characterized by chronic and diffuse non-inflammatory musculoskeletal pain, and FM is often accompanied by fatigue, cognitive disturbances (“fibro fog”), psychiatric symptoms, and multiple other nonspecific somatic symptoms (Galvez-Sánchez & Reyes Del Paso, 2020; Goldenberg, 2022a). Aside from the secondary symptoms, patients may at times experience abdominal and chest wall pain, irritable bowel syndrome (IBS), gastroesophageal reflux disease (GERD), and symptoms of autonomic nervous system (ANS) dysfunction. Despite this, FM is generally of unknown etiology and pathophysiology. However, FM should be considered as a diagnosis in patients experiencing idiopathic chronic pain for at least three months and is solely confirmed by a clinical, symptom-based assessment (D'Agnelli et al., 2019). What adds to the controversial and mysterious nature of the condition is that it depends on subjective symptoms. On a normal physical examination, patients often appear well and do not show abnormalities other than “widespread soft tissue tenderness” with normal laboratory and radiologic studies, making it a common but elusive diagnosis. However, a history of other medical conditions that cause musculoskeletal pain can coexist with or mimic FM like rheumatoid arthritis (RA), systemic lupus erythematosus (SLE), and thyroid disease. Medical history can support a FM diagnosis (Goldenberg, 2022a). FM is more commonly diagnosed in women than men. The prevalence of FM in the United States and other countries is about 2 – 3% and incidence tends to increase with age (Bhargava & Hurley, 2020). FM can also be diagnosed in adolescents in the form of juvenile primary fibromyalgia, and it is confirmed mostly symptomatically but based on slightly different diagnostic criteria for research and epidemiological purposes (Kimura & Walco, 2022).
Fibromyalgia is categorized as a “disorder of pain regulation,” under “central sensitization” (Goldenberg, 2022b). This finding is supported by biochemical abnormalities that are oftentimes present in FM patients: low concentrations of metabolites of serotonin (5HT) and noradrenaline (NA), and high concentrations of substance P and nerve growth factors (Julien et al., 2005). Patients are more sensitive to central nervous system inputs of pain, and those with FM at times can experience symptoms like those suffering from other central pain disorders, like migraines, IBS, and temporomandibular joint disorder (TMD) (Goldenberg, 2022b). Reduced 5HT and NA may actually account for the widespread pain symptoms by contributing to the dysfunction of endogenous systems that inhibit pain sensation (Julien et al., 2005).
Contrary to the established findings published about FM, recent research has demonstrated that there is a possible genetic basis to the disease progression; up to 50% of disease risk can be attributed to candidate genes (D'Agnelli et al., 2019). There also appears to be a strong familial predisposition to FM, although it is suspected to have a more polygenic mode of inheritance (Arnold et al., 2019; Buskila et al., 2007). However, there is no singular definitive gene that directly causes FM; several genes under consideration include SLC64A4, TRPV2, MYT1L, and NRXN3 (D'Agnelli et al., 2019). Single nucleotide polymorphisms (SNPs) in the SLC64A4 gene, which encodes a sodium-dependent serotonin transporter, has been associated with both FM and TMD. SLC64A4 mutations that cause increased serotonin reuptake have been associated with high levels of depression and psychological disorders, as well as “SCL-90 [Symptom Checklist-90 for psychopathological disorders] scores for somatic awareness and anger, TPQ [tridimensional personality questionnaire] harm avoidance trait, increased salivary cortisol level, [and] increased leukocyte count” (D'Agnelli et al., 2019; Diatchenko et al., 2013). TRPV2 (transient receptor potential vanilloid channel 2) gene is needed for not only cell cycle progression, growth, and differentiation of hematopoietic stem cells and innate immunity, but also the pain threshold due to its presence in the mechanoresponsive and thermo-responsive neurons in the dorsal root and trigeminal ganglia (D'Agnelli et al., 2019; Mickle et al., 2015; Santoni et al., 2013). Genetic correlations in FM between mutations in SLC6A4 and TRPV2, which encodes a calcium-permeable channel that is heat-activated and modulates many cellular functions, are further supported by linkage analysis done with FM to the chromosome 17p11.2-q11.2 region, which happens to house the two genes (Arnold et al., 2013; Kojima & Nagasawa, 2014).
Docampo et al. (2014) discovered that the rs11127292 polymorphism in the MYT1L (myelin transcription factor 1 like) gene, which is critical in the process of neuronal differentiation and has historically been associated with neuropsychiatric disorders, and an intronic CNV (copy number variant) in the NRXN3 (neurexin 3) gene, which is involved in signal transmission by promoting synapse stability and function, affect the central nervous system (CNS) aspect of FM as well (Docampo et al., 2014).
Studies have also examined the differences in other allelic frequencies and influence of genetics on the sequelae of FM progression. Smith et al. (2012) identified significant variations in allelic frequency of GABRB3 (rs4906902), TAAR1 (rs8192619), and GBP1 (rs7911) between FM patients and controls. TAAR1 was demonstrated to alter dopamine bioavailability and function, which may cause the increased pain sensitivity seen in FM. RGS4, CNR1, and GRIA4 were implicated in other cohorts from the study by Smith et al. (2012), and are genes primarily involved in mechanisms of analgesia and central sensitivity as well. RGS4, which is expressed in the CNS regions like the dorsal horn of the spinal cord and the locus coeruleus, influences opioid receptor function when overexpressed. CNR1, which encodes the CB-1 cannabinoid receptor, has been indirectly utilized in FM treatment by the cannabinoid receptor agonist nabilone. Low CNR1 expression and thus low CB-1 receptor activity may pose as a strong candidate for future testing, as several FM patients have increased circulating anandamide, an endocannabinoid, which has been hypothesized to underlie the pain in conditions like FM. Alterations to the GRIA4 gene affect AMPA (α-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid) receptors, which play roles in the pain and comorbidities associated with FM (Smith et al., 2012).
Another gene commonly associated with FM is the COMT (catecholamine o-methyl transferase) gene. Though not directly affecting disease presentation, the V158M variant may contribute to subsequent depression, anxiety, and disability in many FM females (D'Agnelli et al., 2019). Mutations in the COMT gene are more closely linked to “pain catastrophizing, increased pain level during elevated pain attention, thermal and pressure sensitivity, psychological distress, increase number of tender points in TPC [tender point count], pain and positive affect interaction, and FIQ [fibromyalgia-impact questionnaire]-defined pain, fatigue, sleep, disturbance, morning stiffness, and disability” (Diatchenko et al., 2013). Similarly, mutations in the HTR2A (5-hydroxytryptamine receptor 2A) gene, which encodes for its receptor, 5-HT2A, contributed to lower levels of total 5-HT in serum and CSF of FM patients (Park & Lee, 2017). The phenotype in FM more closely relates to psychological facets of FM — including reduced perception of environmental quality, “increased SCL-90-R total score and subscales scores for somatic awareness, anxiety, psychosis, obsessive-compulsive behavior, hostility, global severity index, interpersonal sensitivity, phobic anxiety, [and] depression” (Diatchenko et al., 2013).
Research has also demonstrated the role of epigenetics in FM phenotype and progression. Ciampi de Andrade et al. (2017) investigated DNA methylation states in samples obtained from FM cases and healthy controls, and found that the majority (1042 genes, 65%) of the differently methylated genes between the two were mostly hypomethylated. These genes were involved in “transduction and calcium signaling, MAPK signaling pathway, regulation of actin cytoskeleton endocytosis, and neuroactive ligand-receptor interaction pathways,” and the sites that were identified were involved in DNA repair, immune system response and regulation, and membrane transport (D'Agnelli et al., 2019). Additionally, circulating miRNAs obtained from cerebrospinal fluid (CSF) and serum samples were found to be associated with many of the clinical symptoms of FM, including pain and fatigue, alterations in energy metabolism and growth, alterations in pain threshold, and sleep disturbance (Bjersing et al., 2015; Bjersing et al., 2013).
Proprietary Testing
The gradually progressing genetic and epigenetic findings for FM make biomarker testing attractive to researchers and physicians to solidify an alternative nonclinical diagnosis for this debilitating disease. The FM/a® Test takes advantage of the understanding of the immunological biomarkers and genetic components of FM to develop a blood test for diagnosis (FM/a, 2020). Biomarkers assayed through this test were based on a study on levels of cytokines interferon-γ (IFN-γ), interleukin-5 (IL-5), IL-6, IL-8, IL-10, macrophage inflammatory protein-1β (MIP-1β) , monocyte chemoattractant protein-1 (MCP-1), and MIP1-α obtained from samples of plasma and peripheral blood mononuclear cells (PBMC) with/without mitogenic activator treatment (Behm et al., 2012). Results identified that there was no statistically significant difference in these cytokines between FM samples and controls. However, when phytohemagglutinin (PHA), which induces PBMC proliferation and cytokine secretion, phorbol-12-myristate-13-acetate (PMA), and ionomycin, which “stimulate PBMCs and activate extracellular expressions of cytokines,” were cultured with the blood samples, the concentrations of most cytokines in FM samples compared to normal samples were statistically significant, except for IL-5. This immunoassay indicated a connection to the coexisting diagnoses of FM with mental depression and chronic pain, as both these populations tend to experience high pro-inflammatory cytokine levels as well (Behm et al., 2012).
Results supporting the FM/a® Test were further elucidated by Wallace et al. (2015), who looked into the cytokine and chemokine profiles in FM, rheumatoid arthritis, and systemic lupus erythematosus. Using the Luminex multiplex immunoassay bead array technology with mitogenic stimulation of PBMCs, cytokine concentrations for IL-6, IL-8, MIP-a, and MIP-b were recorded. Measures of analytical validity were done using a cytokine/chemokine composite test score. This measurement with all the cytokines/chemokines altogether was considered to have a sensitivity of 93%, a specificity of 89.4%, positive predictive value of 92%, and negative predictive value of 91% for the diagnosis of FM (Wallace et al., 2015).
Other researchers have opted for a proteomics approach to identify individuals with FM. Among females with FMS, Han et al. (2020) discovered dysregulated proteins and mechanisms associated with an FM diagnosis. They propose a panel of methyltransferase-like 18 (METTL18), immunoglobulin lambda variable 3-25 (IGLV3-25), interleukin-1 receptor accessor protein (IL1RAP), and putative V-set and immunoglobulin domain-containing like protein (IGHV1OR21-1) to differentiate FM from healthy controls. This conclusion was drawn from using a decision tree model that yielded an accuracy of 0.97. Collectively, they offered 100% detection sensitivity in their training cohort, and a specificity of 88% (Han et al., 2020).
Genova Diagnostics has also released the NutrEval FMV® Profile, which is a “blood and urine test that evaluates over 125 biomarkers and assesses the body’s functional need for 40 antioxidants, vitamins, minerals, essential fatty acids, amino acids, digestive support, and other select nutrients.” NutrEval® aims to provide insight into conditions such as depression, anxiety, certain inflammatory conditions, and chronic pain syndromes (Genova, 2021). While there are no peer-reviewed studies published to confirm either the analytical or clinical utility of this particular proprietary test, researchers have delved into the biomarkers that comprise this assay. The aforementioned research on COMT proves relevant in the genomics component of this test. The clinical utility for the NutrEval® Profile is particularly pertinent to the chronic pain aspect. In patients with chronic pain, it was found that quinolinic acid, pyroglutamic acid (indicator of glutathione depletion), xanthurenic acid (indicator of vitamin B6 insufficiency), 3-hydroxyropyl mercapturic acid (acrolein metabolite), and methylmalonic acid (indicator of vitamin B12 deficiency) were all elevated to a certain degree among patients experiencing chronic pain. 77% of patients with chronic pain all had at least one abnormal biomarker (Gunn et al., 2020). This demonstrates that understanding the role of nutrition metabolism is necessary for delineating the underlying processes of FM, a chronic pain condition, but additional research is needed.
Clinical Utility and Validity
Currently, most, if not all, of the FM diagnoses are solely clinical. Judgment is made subjectively and dependent on guidelines to conclude if subjective symptoms translate to FM. The sensitivity and specificity of utilizing the 2016 ACR guidelines, when compared to the 1990 criteria in a referral care setting, are 71% and 60%, respectively, with a positive predictive value of 85% and a negative predictive value of 39% (Ahmed et al., 2019). These statistical measures evidently prove that there need be more sensitive and specific measures beyond clinical symptoms for diagnosis of FM.
The clinical utility of an FM diagnosis extends beyond genetic testing and biomarkers; FM is also found concurrently among those with primary immunodeficiency and autoimmune diseases, such as RA, SLE, and Sjögren Syndrome (SS) (Han et al., 2020; Wilke, 1999). Confirming an FM diagnosis could aid in explicating the additional complications found in RA and SLE, such as “alternating constipation and diarrhea, urinary frequency, diffuse paresthesias, and cognitive difficulties.” The converse also holds true — diagnoses of SS could prompt possible FM diagnoses as well, as seen in the cases of seeing sicca symptoms and tender point count of 6 (though not necessary with 2016 ACR guidelines) (Wilke, 1999).
Janssen et al. (2021) conducted a review that identified the polymorphisms related to FM and the respective clinical characteristics. From 27 articles, they found the relevant genes to be MTHFR, RGS4, MYT1L, TACR1, SCN9A, DRD3, ADRB2, IL-4, HLA-DRB1, EDN1, CNR1, TAAR1, OPRM1, ADRA1A, ADRB3, BDNF, GRIA4, HTR3A, HTR3B, HTR2A, SERPINA 1 or A1AT, NRXN3, GCH1, MEFV, TRPV3, SLC6A4, ACE I/D, TSPO, COMT, and MAOA. Additionally, “73.33% of the genes related to FM were also associated with some psychological disorders, such as anxiety, depression, schizophrenia, and obsessive and compulsive disorder, and 40.00% with pain sensitivity and/or migraine, besides other disorders associated (drug addiction, autoimmune disorders, circulatory problems, and metabolic alterations).” Of note, SLC6A4, HTR3A, HTR3B, and HTRA genes were associated with serotonergic regulation, chronic pain conditions, and anxiogenic situations; COMT was related to FM risk and increase in pain severity, increased likelihood of psychological disorders like “depression, anxiety and schizophrenia, alcoholism, opioid addiction, and eating disorders; BDNF was associated with hyperalgesia in FM; and TACR1 was related to dementia and fatigue. As for treating FM, Janssen et al (2021) also found that TAAR1, RGS4, CNR1, GRIA4 may be considered as targets. These collective findings continue to demonstrate the comorbidities associated with FM, and how understanding the genetic bases may aid in preventing and treating additional sequelae" (Janssen et al., 2021).
Kendler et al. (2022) studied the familial genetic risk for functional somatic disorders including internalizing disorders, chronic fatigue syndrome, IBS, and FM. The study included 5,829,186 individuals in Sweden. The authors used a novel method that assessed aggregated risk in first to fifth degree relatives and adjusted for cohabitation. “Patients with FM carry substantial genetic risks not only for FM, but also for pain syndromes and internalizing, autoimmune and sleep disorders.” Overall, patients with FM had a unique family risk genetic score with elevated genetic risk across other disorders; the was a similar but less marked pattern of genetic risks in patients of other functional somatic disorders. The authors suggest that the genetic risk score for FM differentiated it from classic autoimmune disorder and internalizing disorder (Kendler et al., 2022).
American Pain Society
The Analgesic, Anesthetic, and Addiction Clinical Trial Translations Innovations Opportunities and Networks (ACTTION) partnership with the Food and Drug Administration (FDA) and APS created the ACTTION-APS Pain Taxonomy (AAPT) to help standardize clinically useful and consistent diagnoses of chronic pain disorders. First and foremost, all patients must have chronic pain to be diagnosed with FM. The working group members raised a concern of defining FM-pain as by the 1990 ACR criteria (CWP — chronic widespread pain) or the ACR 2010/2016 criteria of multisite pain (MSP), which were distinguished in count (MSP) versus anatomical distribution (CWP) of pain.
To facilitate identifying FM in clinical practice and in research, the AAPT core diagnostic criteria for FM are as follows:
- “MSP defined as 6 or more pain sites from a total of 9 possible sites [head; left arm; right arm; chest; abdomen; upper back and spine; lower back and spine, including buttocks; left leg; and right leg]
- Moderate to severe sleep problems OR fatigue
- MSP plus fatigue or sleep problems must have been present for at least 3 months” (Arnold et al., 2019).
This guideline did not mention genetic testing for FM (Arnold et al., 2019).
American College of Rheumatology (ACR)
In 2016, the ACR published revisions to their 2010/2011 guidelines on preliminary diagnostic criteria for fibromyalgia and measurements of symptom severity. To satisfy a diagnosis of fibromyalgia, a patient must have:
1. “Widespread pain index (WPI) ≥ 7 and symptom severity (SS) scale score ≥ 5 or WPI 4-6 and SS scale score ≥ 9.
2. Generalized pain, defined as pain in at least 4 or 5 regions, must be present. Jaw, chest, and abdominal pain are not included in generalized pain definition.
3. Symptoms have been present at a similar level for at least 3 months.
4. A diagnosis of fibromyalgia is valid irrespective of other diagnoses. A diagnosis of fibromyalgia does not exclude the presence of other clinically important illnesses.”
The table below obtained from the ACR’s publication regarding ascertainment of WPI and SS is shown.
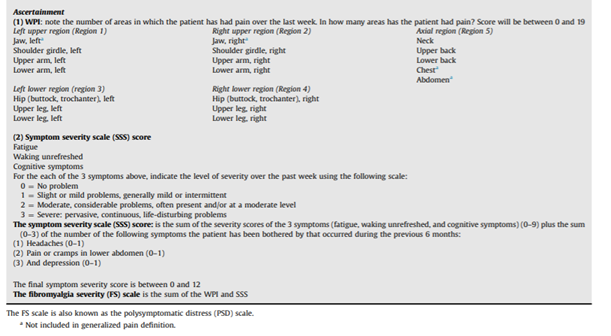
Several cases previously deemed positive by the 2010/2011 criteria would be considered negative by the 2016 modified criteria, indicating a lower specificity. The current criteria also state patients can experience pain in 4 – 5 regions (four quadrants and axial), termed “generalized pain,” to distinguish from the 1990 guideline’s “widespread pain” definition. The 2016 ACR guidelines also now recognize spatial distribution of painful sites (Arnold et al., 2019). It lastly modifies the language from the 2010 guidelines that discuss other disorders serving as the etiology of experienced pain, and assumes the 1990 ACR guideline criterion of possible comorbidities with fibromyalgia (#4) (Wolfe et al., 2016).
After conducting an in-depth review of existing guidelines and literature, Heymann et al. (2017) published recommendations based on the 2010 ACR guidelines, and endorse using the 2010 ACR criteria for diagnosis of FM. They stated:
- “The presence of widespread pain is essential for the diagnosis of patients with suspected FM.
- Tender points may be useful in the diagnosis of fibromyalgia when evaluated in combination with other functional disorders covered in the 2010 [ACR] criteria. The tender point count may be correlated with the intensity of some symptoms, particularly emotional stress.
- Sleep disorders and changes in cognition and fatigue should be considered in the diagnosis of FM. They should also be considered in the assessment of severity of patients with FM.
We suggest the systematic measurement of mood disorders using validated instruments suitable to the healthcare level in which they are administered because they are highly important when assessing the severity of patients with FM” (Heymann et al., 2017).
These guidelines did not mention genetic testing for FM.
Canadian Rheumatology Association (CRA)
The CRA released recommendations to the “identification, evaluation, and management” of those with FM after conducting a needs assessment. In relation to diagnosis of FM, the CRA recommends:
- “Fibromyalgia, a condition that can wax and wane over time, should be diagnosed in an individual with diffuse body pain that has been present for at least 3 months, and who may also have symptoms of fatigue, sleep disturbance, cognitive changes, mood disorder, and other somatic symptoms to variable degree, and when symptoms cannot be explained by some other illness [Level 5, Grade D].
- All patients with a symptom complaint suggesting a diagnosis of fibromyalgia should undergo a physical examination which should be within normal limits except for tenderness on pressure of soft tissues (ie. hyperalgesia which is increased pain following a painful stimulus) [Level 4, Grade D].
- Fibromyalgia should be diagnosed as a clinical construct, without any confirmatory laboratory test, and with testing limited to simple blood testing including a full blood count, erythrocyte sedimentation rate (ESR), C-reactive protein (CRP), creatine kinase, and thyroid stimulating hormone (TSH). Any additional laboratory or radiographic testing should depend on the clinical evaluation in an individual patient that may suggest some other medical condition [Level 5, Grade D]” (Fitzcharles et al., 2012).
References
- Ada. (2020, January 28). Fibromyalgia. Ada Health GmbH. Retrieved January 3 from https://ada.com/conditions/fibromyalgia/
- Ahmed, S., Aggarwal, A., & Lawrence, A. (2019). Performance of the American College of Rheumatology 2016 criteria for fibromyalgia in a referral care setting. Rheumatology International, 39(8), 1397-1403. https://doi.org/10.1007/s00296-019-04323-7
- Arnold, L. M., Bennett, R. M., Crofford, L. J., Dean, L. E., Clauw, D. J., Goldenberg, D. L., Fitzcharles, M.-A., Paiva, E. S., Staud, R., Sarzi-Puttini, P., Buskila, D., & Macfarlane, G. J. (2019). AAPT Diagnostic Criteria for Fibromyalgia. The Journal of Pain, 20(6), 611-628. https://doi.org/https://doi.org/10.1016/j.jpain.2018.10.008
- Arnold, L. M., Fan, J., Russell, I. J., Yunus, M. B., Khan, M. A., Kushner, I., Olson, J. M., & Iyengar, S. K. (2013). The fibromyalgia family study: a genome-wide linkage scan study. Arthritis and rheumatism, 65(4), 1122-1128. https://doi.org/10.1002/art.37842
- Behm, F. G., Gavin, I. M., Karpenko, O., Lindgren, V., Gaitonde, S., Gashkoff, P. A., & Gillis, B. S. (2012). Unique immunologic patterns in fibromyalgia. BMC Clinical Pathology, 12(1), 25. https://doi.org/10.1186/1472-6890-12-25
- Bhargava, J., & Hurley, J. A. (2020). Fibromyalgia. In StatPearls. StatPearls Publishing LLC. https://www.ncbi.nlm.nih.gov/books/NBK540974/
- Bjersing, J. L., Bokarewa, M. I., & Mannerkorpi, K. (2015). Profile of circulating microRNAs in fibromyalgia and their relation to symptom severity: an exploratory study. Rheumatol Int, 35(4), 635-642. https://doi.org/10.1007/s00296-014-3139-3
- Bjersing, J. L., Lundborg, C., Bokarewa, M. I., & Mannerkorpi, K. (2013). Profile of cerebrospinal microRNAs in fibromyalgia. PloS one, 8(10), e78762-e78762. https://doi.org/10.1371/journal.pone.0078762
- Buskila, D., Sarzi-Puttini, P., & Ablin, J. N. (2007). The genetics of fibromyalgia syndrome. Pharmacogenomics, 8(1), 67-74. https://doi.org/10.2217/14622416.8.1.67
- Ciampi de Andrade, D., Maschietto, M., Galhardoni, R., Gouveia, G., Chile, T., Victorino Krepischi, A. C., Dale, C. S., Brunoni, A. R., Parravano, D. C., Cueva Moscoso, A. S., Raicher, I., Kaziyama, H. H. S., Teixeira, M. J., & Brentani, H. P. (2017). Epigenetics insights into chronic pain: DNA hypomethylation in fibromyalgia-a controlled pilot-study. Pain, 158(8), 1473-1480. https://doi.org/10.1097/j.pain.0000000000000932
- D'Agnelli, S., Arendt-Nielsen, L., Gerra, M. C., Zatorri, K., Boggiani, L., Baciarello, M., & Bignami, E. (2019). Fibromyalgia: Genetics and epigenetics insights may provide the basis for the development of diagnostic biomarkers. Molecular pain, 15, 1744806918819944-1744806918819944. https://doi.org/10.1177/1744806918819944
- Diatchenko, L., Fillingim, R. B., Smith, S. B., & Maixner, W. (2013). The phenotypic and genetic signatures of common musculoskeletal pain conditions. Nature Reviews Rheumatology, 9(6), 340-350. https://doi.org/10.1038/nrrheum.2013.43
- Docampo, E., Escaramís, G., Gratacòs, M., Villatoro, S., Puig, A., Kogevinas, M., Collado, A., Carbonell, J., Rivera, J., Vidal, J., Alegre, J., Estivill, X., & Rabionet, R. (2014). Genome-wide analysis of single nucleotide polymorphisms and copy number variants in fibromyalgia suggest a role for the central nervous system. Pain, 155(6), 1102-1109. https://doi.org/10.1016/j.pain.2014.02.016
- Fitzcharles, M. A., Ste-Marie, P. A., Goldenberg, D. L., Pereira, J. X., Abbey, S., Choinière, M., Ko, G., Moulin, D. E., Panopalis, P., Proulx, J., & Shir, Y. (2012, August 17). Canadian Guidelines for the diagnosis and management of fibromyalgia syndrome. Canadian Rheumatology Association. Retrieved January 3 from https://rheum.ca/wp-content/uploads/2017/11/2012CanadianFMGuidelines_17August2012.pdf
- FM/a. (2020). About FM/a. Retrieved January 5 from https://fmtest.com/about-fma/
- Galvez-Sánchez, C. M., & Reyes Del Paso, G. A. (2020). Diagnostic Criteria for Fibromyalgia: Critical Review and Future Perspectives. Journal of clinical medicine, 9(4), 1219. https://doi.org/10.3390/jcm9041219
- Genova. (2021). NutrEval® FMV. Genova Diagnostics. Retrieved January 10 from https://www.gdx.net/product/nutreval-fmv-nutritional-test-blood-urine
- Goldenberg, D. L. (2022a, August 26). Clinical manifestations and diagnosis of fibromyalgia in adults. UpToDate. Retrieved January 3 from https://www.uptodate.com/contents/clinical-manifestations-and-diagnosis-of-fibromyalgia-in-adults
- Goldenberg, D. L. (2022b, September 29). Pathogenesis of fibromyalgia. UpToDate. Retrieved January 4 from https://www.uptodate.com/contents/pathogenesis-of-fibromyalgia
- Gunn, J., Hill, M. M., Cotten, B. M., & Deer, T. R. (2020). An Analysis of Biomarkers in Patients with Chronic Pain. Pain Physician, 23(1), E41-e49.
- Han, C.-L., Sheng, Y.-C., Wang, S.-Y., Chen, Y.-H., & Kang, J.-H. (2020). Serum proteome profiles revealed dysregulated proteins and mechanisms associated with fibromyalgia syndrome in women. Scientific reports, 10(1), 12347-12347. https://doi.org/10.1038/s41598-020-69271-w
- Heymann, R. E., Paiva, E. S., Martinez, J. E., Helfenstein, M., Rezende, M. C., Provenza, J. R., Ranzolin, A., Assis, M. R. d., Feldman, D. P., Ribeiro, L. S., & Souza, E. J. R. (2017). New guidelines for the diagnosis of fibromyalgia. Revista Brasileira de Reumatologia (English Edition), 57, 467-476. https://doi.org/https://doi.org/10.1016/j.rbre.2017.07.002
- Janssen, L. P., Medeiros, L. F., Souza, A., & Silva, J. D. (2021). Fibromyalgia: A Review of Related Polymorphisms and Clinical Relevance. An Acad Bras Cienc, 93(suppl 4), e20210618. https://doi.org/10.1590/0001-3765202120210618
- Julien, N., Goffaux, P., Arsenault, P., & Marchand, S. (2005). Widespread pain in fibromyalgia is related to a deficit of endogenous pain inhibition. Pain, 114(1), 295-302. https://doi.org/https://doi.org/10.1016/j.pain.2004.12.032
- Kendler, K. S., Rosmalen, J. G., Ohlsson, H., Sundquist, J., & Sundquist, K. (2022). A distinctive profile of family genetic risk scores in a Swedish national sample of cases of fibromyalgia, irritable bowel syndrome, and chronic fatigue syndrome compared to rheumatoid arthritis and major depression. Psychological Medicine, 1-8.
- Kimura, Y., & Walco, G. A. (2022, May 10). Fibromyalgia in children and adolescents: clinical manifestations and diagnosis. UpToDate. Retrieved January 3 from https://www.uptodate.com/contents/fibromyalgia-in-children-and-adolescents-clinical-manifestations-and-diagnosis
- Kojima, I., & Nagasawa, M. (2014). TRPV2. Handb Exp Pharmacol, 222, 247-272. https://doi.org/10.1007/978-3-642-54215-2_10
- Mickle, A. D., Shepherd, A. J., & Mohapatra, D. P. (2015). Sensory TRP channels: the key transducers of nociception and pain. Progress in molecular biology and translational science, 131, 73-118. https://doi.org/10.1016/bs.pmbts.2015.01.002
- Park, D.-J., & Lee, S.-S. (2017). New insights into the genetics of fibromyalgia. The Korean journal of internal medicine, 32(6), 984-995. https://doi.org/10.3904/kjim.2016.207
- Santoni, G., Farfariello, V., Liberati, S., Morelli, M. B., Nabissi, M., Santoni, M., & Amantini, C. (2013). The role of transient receptor potential vanilloid type-2 ion channels in innate and adaptive immune responses [Mini Review]. Frontiers in Immunology, 4(34). https://doi.org/10.3389/fimmu.2013.00034
- Smith, S. B., Maixner, D. W., Fillingim, R. B., Slade, G., Gracely, R. H., Ambrose, K., Zaykin, D. V., Hyde, C., John, S., Tan, K., Maixner, W., & Diatchenko, L. (2012). Large candidate gene association study reveals genetic risk factors and therapeutic targets for fibromyalgia. Arthritis and rheumatism, 64(2), 584-593. https://doi.org/10.1002/art.33338
- Wallace, D. J., Gavin, I. M., Karpenko, O., Barkhordar, F., & Gillis, B. S. (2015). Cytokine and chemokine profiles in fibromyalgia, rheumatoid arthritis and systemic lupus erythematosus: a potentially useful tool in differential diagnosis. Rheumatology International, 35(6), 991-996. https://doi.org/10.1007/s00296-014-3172-2
- Wilke, W. S. (1999). The Clinical Utility of Fibromyalgia. JCR: Journal of Clinical Rheumatology, 5(2). https://journals.lww.com/jclinrheum/Fulltext/1999/04000/The_Clinical_Utility_of_Fibromyalgia.11.aspx
- Wolfe, F., Clauw, D. J., Fitzcharles, M.-A., Goldenberg, D. L., Häuser, W., Katz, R. L., Mease, P. J., Russell, A. S., Russell, I. J., & Walitt, B. (2016). 2016 Revisions to the 2010/2011 fibromyalgia diagnostic criteria. Seminars in Arthritis and Rheumatism, 46(3), 319-329. https://doi.org/https://doi.org/10.1016/j.semarthrit.2016.08.012
Coding Section
| Code | Number | Description |
| CPT | 81479 | Unlisted molecular pathology procedure |
| 81599 | Unlisted multianalyte assay with algorithmic analysis | |
| 84999 | Unlisted chemistry procedure |
Procedure and diagnosis codes on Medical Policy documents are included only as a general reference tool for each policy. They may not be all-inclusive.
This medical policy was developed through consideration of peer-reviewed medical literature generally recognized by the relevant medical community, U.S. FDA approval status, nationally accepted standards of medical practice and accepted standards of medical practice in this community, Blue Cross Blue Shield Association technology assessment program (TEC) and other nonaffiliated technology evaluation centers, reference to federal regulations, other plan medical policies, and accredited national guidelines.
"Current Procedural Terminology © American Medical Association. All Rights Reserved"
History From 2020 Forward
| 04/07/2023 | Annual review, no change to policy intent, but, policy being rewritten for clarity and consistency. Also updating description, rationale and reference. |
|
04/22/2022 |
Annual review, no change to policy intent. Updating rationale and references. Adding table of terminology. |
|
04/07/2021 |
New Policy |