
Flow Cytometry - CAM 120
Description
Flow cytometry is a technique for live cell analysis that measures optical light scattering features to determine physical characteristics (Adan et al., 2017). This instrument is beneficial for calculating the number of cells in a biologic sample, as well as for measuring cellular properties, such as size, shape, viability, and granularity (Verbsky & Routes, 2021). Flow cytometry may also be used for diagnostic and prognostic purposes when monitoring certain diseases, and for identifying the presence of specific biomarkers.
Flow cytometry-derived DNA content can be used for cell cycle analysis to estimate the percentages of a cell population in the various phases of the cell cycle; it can also be used with other reagents to analyze only the S phase. A S-phase fraction (SPF) is an assessment of how many cells are actively synthesizing DNA (UIHC, 2016). It is used as a measure of cell proliferation, particularly for cancer (Pinto et al., 1999). A high SPF value is indicative of rapid cancer growth (ACS, 2021).
Policy
Application of medical necessity criteria is dependent upon an individual’s benefit coverage at the time of the request.
- Flow cytometry immunophenotyping of cell surface markers is considered MEDICALLY NECESSARY for any of the following conditions:
- For individuals with cytopenias, lymphomas, leukemia, myeloproliferative and lymphoproliferative disorders, or myelodysplastic syndrome
- For B-cell monitoring for immunosuppressive disorders
- For T-cell monitoring for HIV infection and AIDS
- For individuals with mast cell neoplasms
- For individuals with paroxysmal nocturnal hemoglobinuria
- For post-operative monitoring of members who have undergone organ transplantation
- For individuals with plasma cell disorders
- For individuals with primary immunodeficiencies (PIDs), and PIDs involving T, NK
- For individuals with primary platelet disorders (non-neoplastic)
- For individuals with red cell and white cell disorders (non-neoplastic)
- The following reimbursement limitations will apply for flow cytometry:
- For flow cytometric immunophenotyping for the assessment of potential hematolymphoid neoplasia, use codes 88184 – 88189.
- Code 88184 should be used for the first marker, per specimen, and is reimbursable up to a maximum of two units per date of service.
- Code 88185 should be used for each additional marker and is reimbursable up to a maximum of 35 units, per date of service.
- In patients with a neoplasm with an established immunophenotype, subsequent tests for that neoplasm should be limited to diagnostically relevant markers.
- Codes 88187, 88188, and 88189 should not be used together for a single specimen in any combination.
- Codes 88187, 88188, and 88189 are reimbursed at one unit per specimen, up to two specimens, per date of service.
- Codes 88187 – 88189 should not be used in conjunction with codes 86355, 86356, 86357, 86359, 86360, 86361, 86367.
- Use codes 86355, 86357, 86359, 86360, 86361, or 86367 for cell enumeration. These codes are reimbursable as single units only.
- Coding:
Bill Type Codes
|
012x |
Hospital Inpatient (Medicare Part B only) |
|
013x |
Hospital Outpatient |
|
014x |
Hospital — Laboratory Services Provided to Non-patients |
|
018x |
Hospital — Swing Beds |
|
021x |
Skilled Nursing — Inpatient (Including Medicare Part A) |
|
022x |
Skilled Nursing — Inpatient (Medicare Part B only) |
|
023x |
Skilled Nursing — Outpatient |
|
071x |
Clinic — Rural Health |
|
077x |
Clinic — Federally Qualified Health Center (FQHC) |
|
085x |
Critical Access Hospital |
Group 1 Codes:
|
88182 |
Cell marker study |
|
88184 |
Flowcytometry/ tc 1 marker |
|
88185 |
Flowcytometry/tc add-on |
|
88187 |
Flowcytometry/read 2 – 8 |
|
88188 |
Flowcytometry/read 9 – 15 |
|
88189 |
Flowcytometry/read 16 & > |
Group 2: Quantitative Codes in immunology section
Group 2 Codes:
|
86355 |
B cells total count |
|
86356 |
Mononuclear cell antigen |
|
86357 |
Nk cells total count |
|
86359 |
T cells total count |
|
86360 |
T cell absolute count/ratio |
|
86361 |
T cell absolute count |
|
86367 |
Stem cells total count |
The following does not meet coverage criteria due to a lack of available published scientific literature confirming that the test(s) is/are required and beneficial for the diagnosis and treatment of a patient’s illness.
- Measurement of flow cytometry-derived DNA content (DNA Index) or cell proliferative activity (S-phase fraction or % S-phase) for prognostic or therapeutic purposes in the routine clinical management of cancers is considered NOT MEDICALLY NECESSARY.
Rationale
Flow cytometry is a laboratory technique with the capability to measure optical and fluorescence characteristics from single cells or other particles between 0.2 and 150 micrometers in size, such as microorganisms, nuclei or chromosome preparations suspended in fluid (Brown & Wittwer, 2000; Verbsky & Routes, 2022). More than 100 companies constitute the flow cytometry market, leading to an industry worth of more than $3 billion (Robinson & Roederer, 2015).
A typical flow cytometer contains five main components: a flow cell, a laser, optical parts, detectors which amplify signals, and an electronic or computer system (Verbsky & Routes, 2022). This device measures thousands of cells instantaneously by passing them through the laser beam, and it can even sort the cells into 96- or 384-well plates, tubes, and slides based on identified cellular properties (McKinnon, 2018). Size is determined by the forward angle light scatter, and internal properties such as cellular granularity are measured by the right-angle light scatter (Brown & Wittwer, 2000; Verbsky & Routes, 2022). These fluorescent light signals are converted into electronic signals and then analyzed by a computer to generate final results (McKinnon, 2018).
Fluorescent reagents may be used to enhance a sample before administration into the flow cytometer. These reagents may include DNA binding dyes, fluorescently conjugated antibodies, viability dyes, fluorescent expression proteins, and ion indicator dyes (McKinnon, 2018). Each fluorescent dye binds to cellular components differently, leading to distinguished outcomes when passed by the light source. A fluorochrome, or chemical that can re-emit light when excited, can assist in the detection of specific cellular properties. The use of multiple fluorochromes at once allows several characteristics to be identified instantaneously as different colors emit different wavelengths of light; common dyes include propidium iodide, phycoerythrin, and fluorescein (Brown & Wittwer, 2000).
Immunophenotyping is the most common use of flow cytometry and entails the identification of cellular markers from the immune system, such as T cell subsets and cytokines, as well as antigen-specific responses. Unfortunately, immunophenotyping faces issues in the clinical world due to a lack of standardized procedures (Finak et al., 2016). Current instruments allow for up to 28 colors to be used in immunophenotyping experiments, yet many researchers use less than this (McKinnon, 2018).
Flow cytometry as a laboratory technique can measure and assess DNA ploidy through cell cycle analysis. DNA synthesis and replication errors are associated with cancer. Cancer is the uncontrolled growth and spread of abnormal cells and is increasingly shown to be initiated, propagated, and maintained by somatic genetic events (Johnson et al., 2014).
During the cell cycle, DNA synthesis is tightly regulated and only performed just as the cell is about to divide. This step of DNA replication is called the “S-phase” (Christensen, 2022). Dysfunction of DNA replication is significantly associated with cancer, and cancers frequently involve damage or removal of molecular regulators of replication (Van der Aa et al., 2013). Assessment of the fraction of cells in S-phase has been proposed as an indicator of neoplasm aggression. S-phase fraction (SPF) is thought to reflect proliferative activity of cancer and may provide prognostic or therapeutic information (Ermiah et al., 2012). Elevated proliferative activity may predict a worsened disease-free or overall survival in several cancers, such as breast, non-small cell lung, colorectal, ovarian, kidney, bladder, prostate, and endometrial cancers (Bagwell et al., 2001; Gawrychowski et al., 2003; Kenney et al., 2008; Mangili et al., 2008; Pinto et al., 2011; Ross, 1996). However, data supporting the use of SPF as a prognostic tool appears to be inconsistent at best (Locker et al., 2006).
Clinical Utility and Validity
Technically, any biologic sample can be analyzed by flow cytometry. However, blood is the most common sample type, including both whole blood and peripheral blood mononuclear cells (Verbsky & Routes, 2022). Flow cytometry can be employed for prognostic and diagnostic purposes. This technique has been used to identify both primary immunodeficiencies and secondary or acquired immunodeficiencies such as HIV (Verbsky & Routes, 2022). Primary immunodeficiencies represent more than 300 known genetic disorders, and flow cytometry is a major component of the diagnosis of these disorders (Abraham & Aubert, 2016). Flow cytometry may also be used for prenatal diagnoses, hematology, transplantation, crop improvement, sperm sorting for sex preselection, post-bone marrow transplantation analyses, and during immunosuppression and chemotherapy treatments (Halder et al., 2017; Verbsky & Routes, 2022).
Today, many assays have been developed for flow cytometry purposes. These assays can identify biomarkers for cancer and stem cells, DNA and RNA, reactive oxygen species, and the functional status of yeast or bacteria (Robinson & Roederer, 2015). Newer techniques have also been developed such as mass cytometry: the combination of flow cytometry and mass spectrometry (Cosma et al., 2017). Flow fluorescent in situ hybridization (FISH) is another combinatory technique which is the combination of fluorescent in situ hybridization in suspension (FISHIS) and flow cytometry using DNA or gene-specific probes.
Flow cytometry techniques have been used to identify several types of cancer. Fromm et al. (2009) used flow cytometry to identify classical Hodgkin lymphoma, neoplastic Hodgkin, and Reed Sternberg cells in lymph nodes with 88.7% sensitivity and 100% specificity. Paiva et al. (2016) state that next generation multiparameter flow cytometry “should be considered mandatory in the routine evaluation of multiple myeloma patients both at diagnosis and after therapy and represents an attractive technique to integrate with high-throughput DNA and RNA-seq methods to help in understanding the mechanisms behind dissemination and chemoresistance of multiple myeloma.” Finally, Novikov et al. (2019) used flow cytometry immunophenotyping to identify malignant T-cell clones in mature peripheral T-cell lymphomas with 97% sensitivity and 91% specificity.
Wang et al. (2019) published a study on the applicability of multiparameter (multicolor) flow cytometry (MFC) for detecting MRD to predict relapse in patients with AML after allogeneic transplantation. The researchers also compared MFC to MRD status determined using real-time quantitative polymerase chain reaction (RT-qPCR) from 158 bone marrow samples from 44 different individuals. “Strong concordance was found between MFC-based and RT-qPCR-based MRD status (κ = 0.868).” Moreover, for individuals in complete remission (CR), “the positive MRD status detected using MFC was correlated with a worse prognosis [HRs (P values) for relapse, event-free survival, and overall survival: 4.83 (< 0.001), 2.23 (0.003), and 1.79 (0.049), respectively]; the prognosis was similar to patients with an active disease before HSCT [hematopoietic stem cell transplantation]” (Wang et al., 2019).
Clinical Utility and Validity of DNA Ploidy Cell Cycle Analysis
Carloni et al. (2017) evaluated the associations between SPF and peritoneal carcinomatosis from ovarian cancer. Fifty-three patients were examined, and although SPF differed among the different ploidy categories, no significant correlation was found between SPF and clinical pathological characteristics of patients. However, the authors did find that sensitivity to taxol was correlated with SPF, therefore concluding that “ploidy and SPF could facilitate the choice of therapy for patients with peritoneal carcinomatosis” (Carloni et al., 2017).
Svanvik et al. (2019) examined 1113 patients diagnosed with stage I-III grade 1 – 3 endometrioid endometrial carcinoma in 2006 – 2011. They evaluated both DNA ploidy and SPF and set the SPF cutoff at 8%. The authors found that 5-year relative survival was significantly associated with SPF and DNA ploidy through a univariate statistical analysis. However, when other variables such as age, grade, and stage were added, SPF and DNA ploidy became statistically insignificant. Therefore, the authors concluded that “S-phase fraction, DNA ploidy, and p53 overexpression did not improve identification of high-risk patients by stage, grade, and age in stage I – III endometrioid endometrial carcinoma” (Svanvik et al., 2019).
Thomas et al. (2020) completed a study to analyze the prognostic implications of DNA repair, DNA ploidy and telomerase in the malignant transformation risk assessment of leukoplakia. Samples from 200 patients with oral leukoplakia, 100 patients with oral cancer and 100 healthy controls were analyzed. The DNA ploidy content was measured with high resolution flow cytometry; the authors identified that “There was significant difference in the distribution of ploidy status, telomerase activity and DNA repair capacity among control, leukoplakia and oral cancer group (p < 0.001). When the molecular markers were compared with histological grading of leukoplakia, both DNA ploidy analysis and telomerase activity showed statistical significance (p < 0.001)” (Thomas et al., 2020).
Taniguchi et al. investigated the correlation between flow cytometry parameters such as DNA ploidy, DNA index and S-phase fraction and clinical prognostic factors such as mitotic count and Ki-67 labelling index (LI). The cancer of interest was “gastrointestinal stromal tumours (GIST)” and eighteen specimens from laparoscopic local gastrectomy were analyzed. The authors found these flow cytometry parameters to correlate well with mitotic count ≤ 5 and Ki-67 LI ≤ 6. DNA index was found to be 83.3% accurate in predicting mitotic count ≤ 5 and 77.8% accurate in predicting Ki-67 LI ≤ 6, while S-phase fraction was found to be 94.4% accurate and 88.9% accurate, respectively. The authors concluded that “Rapid flow cytometry parameters can classify risk without the need for histological analysis” (Taniguchi et al., 2021).
Panwar et al. (2021) studied the evaluation of DNA ploidy and S-phase fraction in fine needle aspirates from breast carcinoma. Fifty breast cancer patients who underwent fine needle aspiration cytology (FNAC) were included in the study. The samples from FNAC underwent DNA ploidy and SPF analysis and Ki-67 was estimated. SPF and Ki-67 were compared with each other. "On DNA flow cytometry, 27 (54%) cases were aneuploid and 23 (46%) cases were diploid. The median SPF was 12.43% and 4.03% in aneuploid and diploid tumors respectively. Median Ki-67 among aneuploid tumors was 28.6% compared to 8.7% among diploid tumors. Aneuploid tumors were significantly associated with higher values of SPF and Ki-67, with Kappa 0.437 and agreement of 72%. Diploid tumors showed lower values of SPF and Ki-67, with Kappa 0.455 and agreement of 72.7%. Correlation among SPF and Ki-67 was highly significant with Kappa value 0.446, P value of .002 and agreement of 72.3%" (Panwar et al., 2021). The authors conclude that DNA ploidy and proliferative activity by flow cytometric SPF estimation can provide valuable prognostic information in breast cancer diagnosis.
Flow cytometry is broadly used for many conditions such as cancers, which are mentioned across many different societies. The below section is not a comprehensive list of guidance for flow cytometry.
The European Research Initiative on CLL (ERIC) & European Society for Clinical Cell Analysis (ESCCA) Harmonisation Project
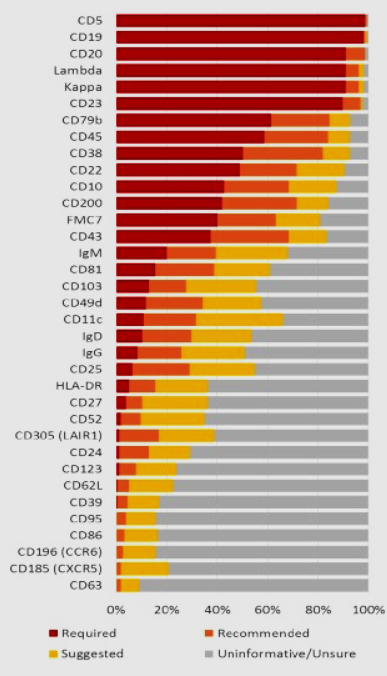
This group has published guidelines on chronic lymphocytic leukemia (CLL) in hopes to determine 35 potential flow cytometry markers as being “required,” “recommended,” “suggested,” “uninformative,” or “not sure” for the diagnosis of CLL (Rawstron et al., 2018). A marker is required if > 75% of ERIC/ESCCA members determine that it should be required, and a marker is pushed forward for review if > 50% of all members determine that it should be recommended or required. Results are shown in the following figure:
Figure 1 [taken from (Rawstron et al., 2018)]:
International/European Leukemia Net Working Group for Flow Cytometry in Myelodysplastic Syndromes
An international working party was organized to develop flow cytometry techniques in the classification of myelodysplastic syndromes (MDS). The group has stated the following guidelines:
- “In laboratories where comprehensive immunophenotyping can be performed, an MDS immunophenotyping panel … is recommended.
- In patients with cytological findings suggesting MDS of RCUD (refractory anemia subtype) or refractory anemia with ringed sideroblasts categories, aberrant flow cytometry (FCM) findings in the granulopoietic or myelomonocytic lineages may indicate multilineage dysplasia, which is of prognostic significance. Morphological findings in these cases should be thoroughly re-evaluated to avoid misclassification.
- It is important to note even small populations of myeloid progenitors with multiple immunophenotypic aberrant features (such as aberrant expression of CD7, CD56 or CD11b, see Table 1), since they indicate a higher risk of progression to AML. FCM findings in these cases should be included in the individual risk assessment” (Porwit et al., 2014).
The Clinical Cytometry Society 2006 Bethesda International Consensus
In 2006, a panel of subject matter experts convened to define the clinical indications that warrant the use of flow cytometry, as well as to identity of the reagents that should be used in the initial and secondary evaluations for those conditions (Davis et al., 2007). The output of that gathering was the 2006 Bethesda International Consensus Recommendations on the Immunophenotypic Analysis of Hematolymphoid Neoplasia by Flow Cytometry. The panel indicated that flow cytometry is useful for the evaluation of cytopenias, elevated leukocyte count, observation of atypical cells or blasts and evaluation of body fluids, plasmacytosis or monoclonal gammopathy, organomegaly and tissue masses, and certain patient monitoring indications.
The Bethesda recommendations indicate that flow cytometry is not indicated for mature neutrophilia, polyclonal hypergammaglobulinemia, polycythemia, thrombocytosis, and basophilia because “they are usually not associated with hematolymphoid malignancy or associated with hematolymphoid neoplasms that are not detectable by” flow cytometry.
The Bethesda recommendations also indicate that selection of reagents for the initial evaluation panel should be based on specimen type (peripheral blood, bone marrow, tissue, etc.), clinical information and cell morphology studies. They identify initial panels for specific indications that range from a total of 4 reagents to a maximum of 12 reagents.
For secondary evaluation, where the initial evaluation is not conclusive or informative, the Bethesda recommendations again identify groups of reagents that should be used, based on indication. The secondary panels ranged from 5 to 23 reagents.
Specific recommendations for the initial evaluation were:
- B cells: CD5, CD10, CD19, CD20, CD45, Kappa, Lambda
- T cells and NK cells: CD2, CD3, CD4, CD5, CD7, CD8, CD45, CD56
- Myelomonocytic cells: CD7, CD11b, CD13, CD14, CD15, CD16, CD33, CD34, CD45, CD56, CD117, HLA-DR
- Myelomonocytic cells (limited): CD13, CD33, CD34, CD45
- Plasma cells CD19, CD38, CD45, CD56
For secondary evaluation, the Bethesda recommendations were:
- B cells: CD9, CD11c, CD15, CD22, cCD22, CD23, CD25, CD13, CD33, CD34, CD38, CD43, CD58, cCD79a, CD79b, CD103, FMC7, Bcl-2, cKappa, cLambda, TdT, Zap-70, cIgM
- T cells and natural killer (NK) cells: CD1a, cCD3, CD10, CD16, CD25, CD26, CD30, CD34, CD45RA, CD45RO, CD57, ab-TCR, gd-TCR, cTIA-1, T-beta chain isoforms, TdT
- Myelomonocytic cells: CD2, CD4, CD25, CD36, CD38, CD41, CD61, cCD61, CD64, CD71, cMPO, CD123, CD163, CD235a
- Plasma cells: CD10, CD117, CD138, cKappa, cLambda
The American Society of Clinical Oncology Tumor Markers Expert Panel (ASCO)
In 2006, the ASCO updated the recommendations for the use of tumor marker tests in the prevention, screening, treatment, and surveillance of gastrointestinal cancers. These recommendations state that “Neither flow-cytometrically derived DNA ploidy (DNA index) nor DNA flow cytometric proliferation analysis (% S phase) should be used to determine prognosis of early-stage colorectal cancer” (Locker et al., 2006).
In 2007, the ASCO updated the recommendations for the use of tumor marker tests in the prevention, screening, treatment, and surveillance of breast cancer (Harris et al., 2007); the authors noted that “DNA/ploidy by flow cytometry demonstrated insufficient evidence to support routine use in clinical practice.”
College of American Pathologists and the American Society of Hematology
In 2016, the College of American Pathologists (CAP) and the American Society of Hematology (ASH) published a joint guideline to outline their recommendations for the initial diagnostic workup of acute leukemia. Among their 27 recommendations, three statements (each rated “Strong Recommendation”) explicitly address the leveraging of flow cytometry in said process:
“5. In addition to morphologic assessment (blood and bone marrow), the pathologist or treating clinician should obtain sufficient samples and perform conventional cytogenetic analysis (i.e., karyotype), appropriate molecular genetic and/or fluorescent in situ hybridization (FISH) testing, and flow cytometric immunophenotyping (FCI). The flow cytometry panel should be sufficient to distinguish acute myeloid leukemia (including acute promyelocytic leukemia), T-cell acute lymphoblastic leukemia (T-ALL) (including early T-cell precursor leukemias), B-cell precursor ALL (B-ALL), and acute leukemia of ambiguous lineage on all patients diagnosed with acute leukemia. FISH and/or molecular genetic testing does not, however, replace conventional cytogenetic analysis.
Note — If sufficient bone marrow aspirate or peripheral blood material is not available for FCI, immunohistochemical studies may be used as an alternative method for performing limited immunophenotyping. In addition, a second bone marrow core biopsy can be obtained and submitted, unfixed in tissue culture media, for disaggregation for genetic studies and flow cytometry.”
“10. For patients with suspected or confirmed acute leukemia, the pathologist may use flow cytometry for the evaluation of CSF.”
“12. For patients with suspected or confirmed acute leukemia, the pathologist or treating clinician should ensure that flow cytometry analysis or molecular characterization is comprehensive enough to allow subsequent detection of minimal residual disease.”
A final recommendation (also a “Strong Recommendation”) mentioning flow cytometry referred to the use of its data, such that
“24. If a patient is referred to another institution for treatment, the primary institution should provide the treatment center with all laboratory results, pathology slides, flow cytometry data, cytogenetic information, and a list of pending tests at the time of the referral. Pending test results should be forwarded when they become available.”
International Society on Thrombosis and Haemostasis (ISTH)
The International Society on Thrombosis and Haemostasis SSC Subcommittee outlined several recommendations for which flow cytometric analysis of inherited and acquired platelet disorders should occur. Those clinical settings in which it believed would be helpful, guided by expert consensus, are reported below:
“Diagnosis of inherited or acquired deficiencies of platelet surface glycoproteins (BSS, GT, inherited or immune-mediated GPVI defects)
Diagnosis of platelet alpha granule secretion defects (such as gray platelet syndrome)
Diagnosis of defects in specific platelet activation (signaling) pathways (such as RASGRP2, P2Y12, or TXA2R disorders)
Diagnosis of GFI1B macrothrombocytopenia associated to platelet expression of CD34
Diagnosis of disorders of platelet procoagulant activity (such as Scott syndrome and Stormorken syndrome)
Assessment of increased platelet activation in prothrombotic syndromes (diabetes, anti-phospholipid syndrome or secondary to drug induced, non-immune platelet activation)
Monitoring, if applicable, pharmacodynamic effect of P2Y12 antagonists (ticlopidine, clopidogrel, prasugrel, ticagrelor, cangrelor) with specifically designed test such as VASP P2Y12
Determination of the fraction of immature platelets” (Frelinger et al., 2021).
National Comprehensive Cancer Network (NCCN)
NCCN clinical practice guidelines on diagnosis and/or management of Breast Cancer (Version 2.2023), Cervical Cancer (Version 1.2023), Colon Cancer (Version 3.2022), Small Cell Lung Cancer (Version 3.2023), and Non-Small Cell Lung Cancer (Version 2.2023) do not mention cell proliferation activity (S-phase fraction or % S-phase) as a management tool (NCCN, 2023).
International Society of Gynecological Pathologists (ISGyP) Endometrial Cancer Project: Guidelines from the Special Techniques and Ancillary Studies Group
These guidelines focus on biomarkers and their potential use for endometrial carcinoma.
The guideline remarks that “Other than markers which are useful in diagnosis, there are few specific studies that provide definitive evidence for the routine use of IHC [immunohistochemistry] or ploidy analysis in determining the prognosis of EC” and that “There is some literature on the association of ploidy with prognosis, with promising results, but there is a lack of definitive studies to determine its true prognostic impact.”
Overall, the guideline states that “Clearly, large prospective, well defined, uniform studies are needed to determine the possible role of IHC for specific biomarkers and ploidy analysis in the clinical setting” (Cho et al., 2019).
Table of Terminology
|
Term |
Definition |
|
AIDS |
Acquired immune deficiency syndrome |
|
AML |
Acute myeloid leukemia |
|
ASCO |
American Society of Clinical Oncology |
|
ASH |
American Society of Hematology |
|
B-ALL |
B-cell precursor ALL |
|
CAP |
College of American Pathologists |
|
CLIA ’88 |
Clinical Laboratory Improvement Amendments of 1988 |
|
CLL |
Chronic lymphocytic leukemia |
|
CMPD |
Chronic myeloproliferative disorders |
|
CMS |
Centers for Medicare & Medicaid |
|
CSF |
Cerebrospinal fluid |
|
DNA |
Deoxyribose nucleic acid |
|
ERIC |
European Research Initiative on CLL |
|
ESCCA |
European Society for Clinical Cell Analysis |
|
FCI |
Flow cytometric immunophenotyping |
|
FCM |
Flow cytometry |
|
FDA |
Food and Drug Administration |
|
FISH |
Fluorescent in situ hybridization |
|
FISHIS |
Fluorescent in situ hybridization in suspension |
|
HIV |
Human immunodeficiency virus infection |
|
HSCT |
Hematopoietic stem cell transplantation |
|
ISTH |
International Society on Thrombosis and Haemostasis |
|
LCDs |
Local coverage determinations |
|
LDTs |
Laboratory developed tests |
|
MDS |
Myelodysplastic syndromes |
|
MFC |
Multiparameter (multicolor) flow cytometry |
|
MRD |
Minimal residual disease |
|
NCDs |
National coverage determinations |
|
NK |
Natural killer |
|
PIDs |
Primary immunodeficiencies |
|
RCUD |
Refractory anemia subtype |
|
RNA |
Ribonucleic acid |
|
RT-qPCR |
Real-time quantitative polymerase chain reaction |
|
T-ALL |
T-cell acute lymphoblastic leukemia |
References
- Abraham, R. S., & Aubert, G. (2016). Flow Cytometry, a Versatile Tool for Diagnosis and Monitoring of Primary Immunodeficiencies. Clin Vaccine Immunol, 23(4), 254-271. https://doi.org/10.1128/cvi.00001-16
- ACS. (2021). Breast Cancer Ploidy and Cell Proliferation. https://www.cancer.org/cancer/breast-cancer/understanding-a-breast-cancer-diagnosis/ploidy-and-cell-proliferation.html
- Adan, A., Alizada, G., Kiraz, Y., Baran, Y., & Nalbant, A. (2017). Flow cytometry: basic principles and applications. Crit Rev Biotechnol, 37(2), 163-176. https://doi.org/10.3109/07388551.2015.1128876
- Bagwell, C. B., Clark, G. M., Spyratos, F., Chassevent, A., Bendahl, P. O., Stal, O., Killander, D., Jourdan, M. L., Romain, S., Hunsberger, B., & Baldetorp, B. (2001). Optimizing flow cytometric DNA ploidy and S-phase fraction as independent prognostic markers for node-negative breast cancer specimens. Cytometry, 46(3), 121-135. https://pubmed.ncbi.nlm.nih.gov/11449403/
- Brown, M., & Wittwer, C. (2000). Flow cytometry: principles and clinical applications in hematology. Clin Chem, 46(8 Pt 2), 1221-1229. http://clinchem.aaccjnls.org/content/46/8/1221
- Carloni, S., Gallerani, G., Tesei, A., Scarpi, E., Verdecchia, G. M., Virzi, S., Fabbri, F., & Arienti, C. (2017). DNA ploidy and S-phase fraction analysis in peritoneal carcinomatosis from ovarian cancer: correlation with clinical pathological factors and response to chemotherapy. Onco Targets Ther, 10, 4657-4664. https://doi.org/10.2147/ott.s141117
- Cho, K. R., Cooper, K., Croce, S., Djordevic, B., Herrington, S., Howitt, B., Hui, P., Ip, P., Koebel, M., Lax, S., Quade, B. J., Shaw, P., Vidal, A., Yemelyanova, A., Clarke, B., Hedrick Ellenson, L., Longacre, T. A., Shih, I. M., McCluggage, W. G., . . . Matias-Guiu, X. (2019). International Society of Gynecological Pathologists (ISGyP) Endometrial Cancer Project: Guidelines From the Special Techniques and Ancillary Studies Group. Int J Gynecol Pathol, 38 Suppl 1(Iss 1 Suppl 1), S114-s122. https://doi.org/10.1097/pgp.0000000000000496
- Christensen, K., Hulick, Peter. (2022). Basic genetics concepts: Chromosomes and cell division. https://www.uptodate.com/contents/basic-genetics-concepts-chromosomes-and-cell-division
- Cosma, A., Nolan, G., & Gaudilliere, B. (2017). Mass cytometry: The time to settle down. Cytometry A, 91(1), 12-13. https://doi.org/10.1002/cyto.a.23032
- Davis, B. H., Holden, J. T., Bene, M. C., Borowitz, M. J., Braylan, R. C., Cornfield, D., Gorczyca, W., Lee, R., Maiese, R., Orfao, A., Wells, D., Wood, B. L., & Stetler-Stevenson, M. (2007). 2006 Bethesda International Consensus recommendations on the flow cytometric immunophenotypic analysis of hematolymphoid neoplasia: medical indications. Cytometry B Clin Cytom, 72 Suppl 1, S5-13. https://doi.org/10.1002/cyto.b.20365
- Ermiah, E., Buhmeida, A., Abdalla, F., Khaled, B. R., Salem, N., Pyrhönen, S., & Collan, Y. (2012). Prognostic value of proliferation markers: immunohistochemical ki-67 expression and cytometric s-phase fraction of women with breast cancer in libya. J Cancer, 3, 421-431. https://doi.org/10.7150/jca.4944
- Finak, G., Langweiler, M., Jaimes, M., Malek, M., Taghiyar, J., Korin, Y., Raddassi, K., Devine, L., Obermoser, G., Pekalski, M. L., Pontikos, N., Diaz, A., Heck, S., Villanova, F., Terrazzini, N., Kern, F., Qian, Y., Stanton, R., Wang, K., . . . McCoy, J. P. (2016). Standardizing Flow Cytometry Immunophenotyping Analysis from the Human ImmunoPhenotyping Consortium. Sci Rep, 6, 20686. https://doi.org/10.1038/srep20686
- Frelinger, A. L., 3rd, Rivera, J., Connor, D. E., Freson, K., Greinacher, A., Harrison, P., Kunishima, S., Lordkipanidzé, M., Michelson, A. D., Ramström, S., & Gresele, P. (2021). Consensus recommendations on flow cytometry for the assessment of inherited and acquired disorders of platelet number and function: Communication from the ISTH SSC Subcommittee on Platelet Physiology. J Thromb Haemost, 19(12), 3193-3202. https://doi.org/10.1111/jth.15526
- Fromm, J. R., Thomas, A., & Wood, B. L. (2009). Flow cytometry can diagnose classical hodgkin lymphoma in lymph nodes with high sensitivity and specificity. Am J Clin Pathol, 131(3), 322-332. https://doi.org/10.1309/ajcpw3un9dyldspb
- Gawrychowski, J., Lackowska, B., & Gabriel, A. (2003). Prognosis of the surgical treatment of patients with non-small cell lung cancer (NSCLC)--relation to DNA ploidy. Eur J Cardiothorac Surg, 23(6), 870-877; discussion 877. https://pubmed.ncbi.nlm.nih.gov/12829060/
- Halder, M., Nath, S., & Jha, S. (2017). Flow Cytometry and Its Utility. Chromosome Structure and Aberrations, 109-126. https://link.springer.com/chapter/10.1007/978-81-322-3673-3_5
- Harris, L., Fritsche, H., Mennel, R., Norton, L., Ravdin, P., Taube, S., Somerfield, M. R., Hayes, D. F., & Bast, R. C., Jr. (2007). American Society of Clinical Oncology 2007 update of recommendations for the use of tumor markers in breast cancer. J Clin Oncol, 25(33), 5287-5312. https://doi.org/10.1200/jco.2007.14.2364
- Johnson, D. B., Dahlman, K. H., Knol, J., Gilbert, J., Puzanov, I., Means-Powell, J., Balko, J. M., Lovly, C. M., Murphy, B. A., Goff, L. W., Abramson, V. G., Crispens, M. A., Mayer, I. A., Berlin, J. D., Horn, L., Keedy, V. L., Reddy, N. M., Arteaga, C. L., Sosman, J. A., & Pao, W. (2014). Enabling a Genetically Informed Approach to Cancer Medicine: A Retrospective Evaluation of the Impact of Comprehensive Tumor Profiling Using a Targeted Next-Generation Sequencing Panel. Oncologist, 19(6), 616-622. https://doi.org/10.1634/theoncologist.2014-0011
- Kenney, B., Zieske, A., Rinder, H., & Smith, B. (2008). DNA ploidy analysis as an adjunct for the detection of relapse in B-lineage acute lymphoblastic leukemia. Leuk Lymphoma, 49(1), 42-48. https://doi.org/10.1080/10428190701760052
- Locker, G. Y., Hamilton, S., Harris, J., Jessup, J. M., Kemeny, N., Macdonald, J. S., Somerfield, M. R., Hayes, D. F., & Bast, R. C., Jr. (2006). ASCO 2006 update of recommendations for the use of tumor markers in gastrointestinal cancer. J Clin Oncol, 24(33), 5313-5327. https://doi.org/10.1200/jco.2006.08.2644
- Mangili, G., Montoli, S., De Marzi, P., Sassi, I., Aletti, G., & Taccagni, G. (2008). The role of DNA ploidy in postoperative management of stage I endometrial cancer. Ann Oncol, 19(7), 1278-1283. https://doi.org/10.1093/annonc/mdn041
- McKinnon, K. M. (2018). Flow Cytometry: An Overview. Curr Protoc Immunol, 120, 5.1.1-5.1.11. https://doi.org/10.1002/cpim.40
- NCCN. (2023). NCCN Clinical Practice Guidelines in Oncology https://www.nccn.org/professionals/physician_gls/default.aspx
- Novikov, N. D., Griffin, G. K., Dudley, G., Drew, M., Rojas-Rudilla, V., Lindeman, N. I., & Dorfman, D. M. (2019). Utility of a Simple and Robust Flow Cytometry Assay for Rapid Clonality Testing in Mature Peripheral T-Cell Lymphomas. Am J Clin Pathol, 151(5), 494-503. https://doi.org/10.1093/ajcp/aqy173
- Paiva, B., Merino, J., & San Miguel, J. F. (2016). Utility of flow cytometry studies in the management of patients with multiple myeloma. Curr Opin Oncol, 28(6), 511-517. https://doi.org/10.1097/cco.0000000000000331
- Panwar, S., Handa, U., Kaur, M., Mohan, H., & Attri, A. K. (2021). Evaluation of DNA ploidy and S-phase fraction in fine needle aspirates from breast carcinoma. Diagn Cytopathol, 49(6), 761-767. https://doi.org/10.1002/dc.24738
- Pinto, A. E., André, S., & Soares, J. (1999). Short-term significance of DNA ploidy and cell proliferation in breast carcinoma: a multivariate analysis of prognostic markers in a series of 308 patients. Journal of Clinical Pathology, 52(8), 604. https://doi.org/10.1136/jcp.52.8.604
- Pinto, A. E., Pires, A., Silva, G., Bicho, C., Andre, S., & Soares, J. (2011). Ploidy and S-phase fraction as predictive markers of response to radiotherapy in cervical cancer. Pathol Res Pract, 207(10), 623-627. https://doi.org/10.1016/j.prp.2011.07.007
- Porwit, A., van de Loosdrecht, A. A., Bettelheim, P., Brodersen, L. E., Burbury, K., Cremers, E., Della Porta, M. G., Ireland, R., Johansson, U., Matarraz, S., Ogata, K., Orfao, A., Preijers, F., Psarra, K., Subira, D., Valent, P., van der Velden, V. H., Wells, D., Westers, T. M., . . . Bene, M. C. (2014). Revisiting guidelines for integration of flow cytometry results in the WHO classification of myelodysplastic syndromes-proposal from the International/European LeukemiaNet Working Group for Flow Cytometry in MDS. Leukemia, 28(9), 1793-1798. https://doi.org/10.1038/leu.2014.191
- Rawstron, A. C., Kreuzer, K. A., Soosapilla, A., Spacek, M., Stehlikova, O., Gambell, P., McIver-Brown, N., Villamor, N., Psarra, K., Arroz, M., Milani, R., de la Serna, J., Cedena, M. T., Jaksic, O., Nomdedeu, J., Moreno, C., Rigolin, G. M., Cuneo, A., Johansen, P., . . . Montserrat, E. (2018). Reproducible diagnosis of chronic lymphocytic leukemia by flow cytometry: An European Research Initiative on CLL (ERIC) & European Society for Clinical Cell Analysis (ESCCA) Harmonisation project. Cytometry B Clin Cytom, 94(1), 121-128. https://doi.org/10.1002/cyto.b.21595
- Robinson, J. P., & Roederer, M. (2015). HISTORY OF SCIENCE. Flow cytometry strikes gold. Science, 350(6262), 739-740. https://doi.org/10.1126/science.aad6770
- Ross, J. S. (1996). DNA ploidy and cell cycle analysis in cancer diagnosis and prognosis. Oncology (Williston Park), 10(6), 867-882, 887; discussion 887-890. https://www.cancernetwork.com/view/dna-ploidy-and-cell-cycle-analysis-cancer-diagnosis-and-prognosis
- Svanvik, T., Stromberg, U., Holmberg, E., Marcickiewicz, J., & Sundfeldt, K. (2019). DNA ploidy status, S-phase fraction, and p53 are not independent prognostic factors for survival in endometrioid endometrial carcinoma FIGO stage I-III. Int J Gynecol Cancer. https://doi.org/10.1136/ijgc-2018-000082
- Taniguchi, K., Suzuki, A., Serizawa, A., Kotake, S., Ito, S., Suzuki, K., Yamada, T., Noguchi, T., Amano, K., Ota, M., Muragaki, Y., & Yamamoto, M. (2021). Rapid Flow Cytometry of Gastrointestinal Stromal Tumours Closely Matches the Modified Fletcher Classification. Anticancer Res, 41(1), 131-136. https://doi.org/10.21873/anticanres.14758
- Thomas, G., Tr, S., George, S. P., Somanathan, T., Sarojam, S., Krishnankutti, N., Sreedharan, H., & Ankathil, R. (2020). Prognostic Implications of DNA Repair, Ploidy and Telomerase in the Malignant Transformation Risk Assessment of Leukoplakia. Asian Pac J Cancer Prev, 21(2), 309-316. https://doi.org/10.31557/apjcp.2020.21.2.309
- UIHC. (2016). Cancer diagnostic tests and blood tests word list. https://uihc.org/health-topics/cancer-diagnostic-tests-and-blood-tests-word-list
- Van der Aa, N., Cheng, J., Mateiu, L., Zamani Esteki, M., Kumar, P., Dimitriadou, E., Vanneste, E., Moreau, Y., Vermeesch, J. R., & Voet, T. (2013). Genome-wide copy number profiling of single cells in S-phase reveals DNA-replication domains. Nucleic Acids Res, 41(6), e66. https://doi.org/10.1093/nar/gks1352
- Verbsky, J., & Routes, J. (2022, 6/7/21). Flow cytometry for the diagnosis of primary immunodeficiencies. https://www.uptodate.com/contents/flow-cytometry-for-the-diagnosis-of-primary-immunodeficiencies
- Wang, Z., Guo, M., Zhang, Y., Xu, S., Cheng, H., Wu, J., Zhang, W., Hu, X., Yang, J., Wang, J., & Tang, G. (2019). The applicability of multiparameter flow cytometry for the detection of minimal residual disease using different-from-normal panels to predict relapse in patients with acute myeloid leukemia after allogeneic transplantation. Int J Lab Hematol, 41(5), 607-614. https://doi.org/10.1111/ijlh.13070
Coding Section
| Codes | Number | Description |
| CPT | 88182 | Flow Cytometry, cell cycle or DNA analysis |
| 88184 | Flow cytometry, cell surface, cytoplasmic, or nuclear marker, technical component only; first marker | |
| 88185 | each additional marker (List separately in addition to code for first marker) | |
| 88187 | Flow cytometry, interpretation; 2 to 8 markers | |
| 88188 | 9 to 15 markers | |
| 88189 | 16 or more markers | |
| 88199 | Unlisted cytopathology procedure | |
| 86355 | B cells, total count | |
| 86356 | Mononuclear cell antigen, quantitative (e.g., flow cytometry), not otherwise specified, each antigen | |
| 86357 | Natural killer (NK) cells, total count | |
| 86359 | T cells; total count | |
| 86360 | Absolute CD4 and CD8 count, including ratio | |
| 86361 | Absolute CD4 count | |
| 86367 | Stem cells (e.g., CD34), total count | |
| 88182 | Flow cytometry, cell cycle or DNA analysis | |
| 88184 | Flow cytometry, cell surface, cytoplasmic, or nuclear marker, technical component only; first marker | |
| 88185 | Flow cytometry, cell surface, cytoplasmic, or nuclear marker, technical component only; each additional marker (List separately in addition to code for first marker) | |
| 88187 | Flow cytometry, interpretation; 2 to 8 markers | |
| 88188 | Flow cytometry, interpretation; 9 to 15 markers | |
| 88189 | Flow cytometry, interpretation; 16 or more markers | |
| ICD-10-CM | C43.111 – C43.122 | Malignant melanoma of right upper eyelid, including canthus |
| O01.0 | Classic hydatidiform mole — Hydatidiform mole, unspecified | |
| O01.1 | Incomplete and partial hydatidiform mole | |
| D04.10 | Carcinoma in situ of skin of eyelid, including canthus | |
| All D37 codes | Neoplasm of uncertain behavior of oral cavity and digestive organs | |
| D81.30 (EFFECTIVE 10/01/2019) | Adenosine deaminase deficiency, unspecified | |
| D81.31 (EFFECTIVE 10/01/2019) | Severe combined immunodeficiency due to adenosine deaminase deficiency | |
| D81.32 (EFFECTIVE 10/01/2019) | Adenosine deaminase 2 deficiency | |
| D81.39 (EFFECTIVE 10/01/2019) | Adenosine deaminase 2 deficiency | |
| R89.7 | Abnormal histological findings in specimens from other organs, systems and tissues | |
| E88.09 | Other disorders of plasma-protein metabolism, not elsewhere classified |
Procedure and diagnosis codes on Medical Policy documents are included only as a general reference tool for each policy. They may not be all-inclusive.
This medical policy was developed through consideration of peer-reviewed medical literature generally recognized by the relevant medical community, U.S. FDA approval status, nationally accepted standards of medical practice and accepted standards of medical practice in this community, Blue Cross Blue Shield Association technology assessment program (TEC) and other nonaffiliated technology evaluation centers, reference to federal regulations, other plan medical policies and accredited national guidelines.
"Current Procedural Terminology © American Medical Association. All Rights Reserved"
History From 2015 Forward
| 04/25/2023 | Annual review, no change in policy intent, but, policy is being rewritten for clarity and consistency. Also updating rationale, references and coding notes. |
| 08/10/2022 | Interim review, adding coverage criteria 1i and 2f. Also updating description, rationale and references. This policy has been merged with the now archived CAM 154 DNA Ploidy Cell Cycle Analysis. |
|
04/19/2022 |
Annual review, adding myeloproliferative disorders to criteria # 1, removing hypercellular hematolymphoid disorders, CLL and CMPD as they are repetitive. Also updating rationale, references, and coding. Adding table of terminology. |
|
04/06/2021 |
Annual review, updating units available per dates of service. Also updating rationale and references. |
|
04/08/2020 |
Annual review, no change to policy intent. |
|
09/24/2019 |
Updated coding. No other changes made. |
|
04/02/2019 |
Annual review, no change to policy intent. Updating coding. |
|
04/18/2018 |
Annual review, no change to policy intent. |
|
04/25/2017 |
Updated category to Laboratory. No other changes. |
|
04/17/2017 |
Annual review, no change to policy intent. |
|
01/31/2017 |
Interim review, updating the number of allowable units of 88185 to be 24 and any numbers greater than 24 will require prior authorization. |
|
01/03/2017 |
Annual review, no change to policy intent. |
|
04/11/2016 |
Interim review to add additional diagnoses that are medically necessary. |
|
12/21/2015 |
NEW POLICY |