
Urine Culture Testing for Bacteria - CAM 206
Description
Bacteriuria is the presence of bacteria in the urine. Urinary tract infections (UTIs) can occur in the urinary system and can be either symptomatic or asymptomatic. UTIs can include cystitis, an infection of the bladder or lower urinary tract; pyelonephritis, an infection of the upper urinary tract or kidney; urosepsis; urethritis; and male-specific conditions, such as bacterial prostatitis and epididymitis (Bonkat et al., 2022; Hooton & Gupta, 2021). Typically, in an infected person, bacteriuria, and pyuria (the presence of pus in the urine) are present and can be present in both symptomatic and asymptomatic UTIs. A urine culture can be performed to determine the presence of bacteria and to characterize the bacterial infection (Meyrier, 2021).
Regulatory Status
Since 1978, the FDA has approved several urine culture kits and devices (FDA, 2018). Additionally, many labs have developed specific urine culture tests that they must validate and perform in house. These laboratory-developed tests (LDTs) are regulated by the Centers for Medicare & Medicaid Services (CMS) as high-complexity tests under the Clinical Laboratory Improvement Amendments of 1988 (CLIA ’88). As an LDT, the U.S. Food and Drug Administration has not approved or cleared this test; however, FDA clearance or approval is not currently required for clinical use.
Policy
- In pregnant individuals, urine culture testing (with isolate identification and antibiotic susceptibilities if applicable) for any urinary tract infection, asymptomatic or symptomatic, including suspected cystitis, pyelonephritis, and asymptomatic bacteriuria, is considered MEDICALLY NECESSARY.
- Prior to undergoing urological interventions which breach the mucosa, urine culture testing (with isolate identification and antibiotic susceptibilities if applicable) in asymptomatic patients is considered MEDICALLY NECESSARY.
- For patients exhibiting at least one sign or symptom of a possible UTI or bacteriuria* (See Note 1 below), urine culture testing (with isolate identification and antibiotic susceptibilities if applicable) is considered MEDICALLY NECESSARY.
- To assess pyelonephritis, urine culture testing (with isolate identification and antibiotic susceptibilities if applicable) is considered MEDICALLY NECESSARY.
- For asymptomatic urinary tract infection or asymptomatic bacteriuria in all other instances, urine culture testing (with isolate identification and antibiotic susceptibilities if applicable) is considered NOT MEDICALLY NECESSARY.
- Follow-up urine culture testing for an uncomplicated urinary tract infection in patients that show evidence of clinical resolution of infection is considered NOT MEDICALLY NECESSARY.
The following does not meet coverage criteria due to a lack of available published scientific literature confirming that the test(s) is/are required and beneficial for the diagnosis and treatment of a patient’s illness.
- Urine culture testing (with isolate identification and antibiotic susceptibilities if applicable) is considered NOT MEDICALLY NECESSARY in the following situations:
- As part of initial screening for asymptomatic prostatitis; OR
- As part of assessment or prognosis of prostate biopsy
*Note 1: Signs and symptoms of UTI/bacteriuria include the following: (CDC, 2019)
-
Fever
-
Urgency to urinate
-
Feeling the need to urinate despite having an empty bladder
-
Increased frequency of urination
-
Dysuria
-
Suprapubic tenderness
-
Pyuria
-
Hematuria
-
Cloudy urine
-
Lower Back and Side (flank) pain
-
Nausea
-
Vomiting
-
Chills
-
Night sweats
-
Pelvic pressure
-
Change in urine smell
-
Abnormal urinalysis findings
Rationale
Urinary tract infections (UTIs) can be either symptomatic or asymptomatic and can be classified as uncomplicated or complicated. Uncomplicated UTIs are “acute, sporadic or recurrent cystitis limited to non-pregnant women with no known relevant anatomical and functional abnormalities within the urinary tract or comorbidities” (Bonkat et al., 2022). All other UTIs that are not defined as uncomplicated are complicated UTIs. Complicated UTIs include “UTIs in a patient with an increased chance of a complicated course: i.e. all men, pregnant [individuals], patients with relevant anatomical or functional abnormalities of the urinary tract, indwelling urinary catheters, renal diseases, and/or with other concomitant immunocompromising diseases for example, diabetes” (Bonkat et al., 2022). Escherichia coli is the most common cause of complicated UTIs; however, “other uropathogens include other Enterobacteriaceae (such as Klebsiella spp and Proteus spp), Pseudomonas, enterococci, and staphylococci (methicillin-sensitive Staphylococcus aureus [MSSA] and methicillin-resistant S. aureus [MRSA])” (Hooton & Gupta, 2021). Even though both bacteriuria and pyuria are often present in UTIs, their presence alone is not indicative of a symptomatic infection.
The presence of bacteriuria does not guarantee negative outcomes for a patient. In fact, the paradigm of the sterility of the bladder environment has changed considerably over recent years. At least for females, the presence of female urinary microbiota (FUM) is believed to occur naturally and has been documented using sensitive bacterial DNA screening tests on asymptomatic females (Brubaker & Wolfe, 2016). Beneficial microbes, such as vaginal strains of Lactobacillus, can inhibit the grown of uropathogenic bacteria, including E. coli (Aroutcheva et al., 2001; Brubaker & Wolfe, 2016). Over-prescribing antibiotics, especially in cases of asymptomatic bacteriuria, can lead to both an eradication of beneficial bacterial flora and an emergence of antibiotic-resistant bacteria. Prescribing antibiotics as a prophylactic measure or in the instance of asymptomatic bacteriuria is detrimental because it is of limited value and can also increase incidences of drug-resistance. A study in 2002 by Harding and colleagues show that antibiotic treatment in diabetic women with asymptomatic bacteriuria did not result in a decrease of future symptomatic UTIs as compared to the control group; in fact, the experimental group had higher rates of adverse antimicrobial reactions (Harding et al., 2002). Even though the evidence-based guidelines by various societies, such as the EAU (Bonkat et al., 2022) and SHEA (SHEA, 2019), do not recommend performing urine testing or treatment for asymptomatic bacteriuria, inappropriate treatment is still occurring; in fact, one study by Cope and colleagues show that 32% of catheter-associated cases of asymptomatic bacteriuria and asymptomatic UTI received inappropriate treatment (Cope et al., 2009). The Antimicrobial Resistance Epidemiological Survey on Cystitis (ARESC) shows that up to 10.3% of E. coli in UTIs are “resistant to at least three different classes of antimicrobial agents” with ampicillin having the highest degree of resistance (48.3%). This is a large study of 4264 women from ten different countries to show that antibiotic-resistance is of international importance (Schito et al., 2009).
Analytical Validity
Urinalysis (UA) to detect nitrite and leukocyte esterase to indicate the presence of bacteria is an accepted laboratory practice. One report, though, has shown that the use of nitrite has “a sensitivity of 3%, a specificity of 97%, and a negative predictive value of 55%” (Cooper et al., 1992). A 2004 meta-analysis study asserts that the “sensitivities of the combination of both tests vary between 68 and 88% in different patient groups, but positive test results have to be confirmed” (Devillé et al., 2004). They did note that the accuracy of the leukocyte esterase testing was higher in urology patients with a diagnostic odds ratio (DOR) of 276 as compared to the accuracy of nitrites (for example, in elderly patients DOR = 108) (Devillé et al., 2004).
Urine culture is considered a “gold standard” for detecting the presence of bacteria in urine (Graham & Galloway, 2001; Schmiemann et al., 2010). That being said, “the interpretation of culture results can be considered as more of an art than a science. A urine culture result depends on so many variables, such as appropriate collection, transport, and the limits of the methods of detection. The reliability of single positive urine culture in diagnosing UTI is only 80%, rising to 90% if a repeat culture shows identical results (Graham & Galloway, 2001).” This is using the definition of bacteriuria as being 105 bacteria/ml of urine.
A potential future alternative to the urine culture could be multiplex PCR-based molecular testing, which Wojno et al. (2020) had found to be noninferior to urine culture for detection and identification of the bacteria. Agreement between the two testing methods was 90%, which exceeded the 85% noninferiority threshold. The multiplex PCR was also able to detect bacteria in 36% of symptomatic patients who had negative urine cultures and detected more polymicrobial infections than urine culture in a shorter amount of time (6 hours vs 48 hours for urine culture) (Wojno et al., 2020).
Clinical Utility and Validity
A study in 2010 (Bruyere et al., 2010) using 353 patients undergoing prostate biopsy show that the routine use of obtaining a pre-operative urine culture is not clinically relevant to positive outcomes. “Of the 353 men, 12 had a pre-biopsy-positive bacterial culture and underwent prostate biopsy without any infections complication. Fifteen patients with a negative pre-biopsy culture developed a post-biopsy-positive bacterial culture, but remained asymptomatic without any treatment. Only four men from the group without pre-biopsy bacteriuria developed an infectious complication, requiring 3 weeks of antibiotic therapy.” Both experimental and control groups had similar rates of complication, suggesting “that routine urine bacterial culture before prostate biopsy is not useful when antibiotic prophylaxis and enema are performed” (Bruyere et al., 2010).
The method of obtaining the urine sample for culture testing is important. This is especially true for children. A 2017 study of 4808 acutely ill children demonstrated that there was modest agreement between the results obtained if the test was conducted by a research laboratory versus a health service laboratory; however, the method of obtaining the urine sample did have significance. The calculated areas under the receiver-operator curve (AUC) for UTI ranged from 0.75-0.86 if the sample was obtained using a clean-catch method versus AUC values of 0.65-0.79 if the sample was obtained using “nappy pad samples”. The authors conclusions were that urine cultures did not necessarily have to be sent to a research lab for testing, but that “primary care clinicians should try to obtain clean catch samples, even in very young children” (Birnie et al., 2017). A smaller study of 83 infants compared the use of urine obtained either via bladder catheterization or suprapubic aspiration (SPA) (Eliacik et al., 2016). All 83 infants had previously tested positive using urine culture samples obtained via bladder catheterization. Then, they had samples removed by SPA. The SPA samples were used in both urinalysis and urine culture testing, and “only 24 (28.9%) and 20 (24%) yielded positive urine culture and abnormal urinalysis data, respectively.” This indicates a 71.1% false-positive result rate if the urine sample is obtained using bladder catheterization. “In infants younger than 12 months, SPA is the best method to avoid bacterial contamination, showing better results than transurethral catheterization” (Eliacik et al., 2016).
Another study (Ducharme et al., 2007) researched the use of either urine cultures and/or reagent test strips for use in diagnosing UTIs in elderly patients. The study consisted of 100 elderly patients with one group having no symptoms and non-infectious complaints and a second group “presenting with acute confusion, weakness or fever but no apparent urinary symptoms.” Their results show that “of the 33 positive cultures, 10 had negative reagent strips. Thirteen of the 14 positive nitrite tests were culture positive for a specificity of 92.8% and a sensitivity of 36.1%. Positive cultures did not infer a diagnosis of UTI. Of the 67 positive reagent strips, 41 (61.2%) were associated with negative cultures.” They conclude that, “in the elderly, reagent testing is an unreliable method of identifying patients with positive blood cultures. Moreover, positive urine culture rates are only slightly higher in patients with vague symptoms attributable to UTI than they are in (asymptomatic) patients treated for non-urologic problems, which suggests that many positive cultures in elderly patients with non-focal systemic symptoms are false-positive tests reflecting asymptomatic bacteriuria and not UTIs” (Ducharme et al., 2007).
A study by Price and colleagues (2016) show that using an enhanced quantitative urine culture (EQUC) increased the detection of microorganisms in UTIs. This study consisted of 150 female patients using an initial UTI symptom assessment questionnaire to divide them into symptomatic and asymptomatic groups. Both sets underwent culture testing using both conventional urine culture testing and an EQUC method. “Compared to expanded-spectrum EQUC, standard urine culture missed 67% of uropathogens overall and 50% in participants with severe urinary symptoms. Thirty-six percent of participants with missed uropathogens reported no symptom resolution after treatment by standard urine culture results.” Their protocol resulted in an “84% uropathogen detection relative to 33% detection by standard urine culture” (Price et al., 2016).
Cantey et al. (2015) evaluated the utility of a Gram stain relative to UA. In reviewing 312 pediatric patients with suspected UTIs who had urine cultures, UA, and Gram stain performed, the researchers concluded that the UA “has excellent negative predictive value that is not enhanced by urine Gram stain and that antibiotic selection did not vary based on the urine Gram stain result.” When compared to the urine Gram stain, the UA had equal sensitivity (97.3% vs 97.5%) and a higher specificity (85% vs 74%). This could allow the UA to take precedent as a test performed over the Gram stain due to its increased efficiency and lower cost (Cantey et al., 2015).
Petty et al. (2019) evaluated the risk factors and clinical outcomes of treating asymptomatic bacteriuria (ASB) in hospitalized patients. 2733 patients with ASB (defined as “positive urine culture without any documented signs or symptoms attributable to urinary tract infection”) were included. 2259 patients were treated with antibiotics for a mean of 7 days. Certain characteristics tended to correlate with ASB treatment, such as positive urinalysis (odds ratio [OR] = 2.83), leukocytosis (OR = 1.55), and dementia (OR = 1.57). However, treatment of ASB was found to be associated with longer duration of hospitalization after urine testing (4 vs 3 days; relative risk, 1.37), although no other differences in secondary outcomes were identified. The authors concluded that “hospitalized patients with ASB commonly receive inappropriate antibiotic therapy. Antibiotic treatment did not appear to be associated with improved outcomes; rather, treatment may be associated with longer duration of hospitalization after urine testing.” The authors also recommended stewardship efforts to reduce inappropriate treatment (Petty et al., 2019).
Coussement et al. (2019) investigated the prevalence of asymptomatic bacteriuria among kidney transplant patients beyond two months post-transplant. The authors identified 500 post-transplant patients, of which 17 had asymptomatic bacteriuria (3.4%). Further, of the 76 patients that were 2-12 months post-transplant, only 1 had asymptomatic bacteriuria, and of the other 424 patients, 16 patients had asymptomatic bacteriuria. The authors concluded that the prevalence of asymptomatic bacteriuria past the second month of kidney transplant was low and that further studies were needed to ascertain the cost-effectiveness of the screen-and-treat strategy in this population (Coussement et al., 2019). This finding regarding screening and treating ASB was confirmed by Fontserè et al. (2021), who found that the “treatment of A[S]B diminished the microbiological cure and increased the rates of microbiologic relapses and reinfections… treated A[S]B patients showed a trend of developing symptomatic urinary tract infection in the following six months.”
Choosing Wisely
Choosing Wisely, an initiative by the American Board of Internal Medicine (ABIM) Foundation, consists of several national organizations representing medical specialists that write recommendations within their respective field to help choose care based on scientific evidence and to help reduce testing redundancy.
2019 AMDA-The Society for Post-Acute and Long-Term Care Medicine (AMDA)
In 2019, the AMDA updated their earlier 2017 Choosing Wisely guideline concerning the use of urine cultures. Due to overuse of antibiotics and overtreatment of UTIs, they state “Don’t obtain urine tests until clinical criteria are met.” Since the urine culture would have a high likelihood of yielding a positive result in an otherwise asymptomatic case, this “contributes to the over-use of antibiotic therapy in this setting, leading to an increased risk of diarrhea or other adverse drug events, resistant organisms and infection due to Clostridioides difficile.” They also note that “the finding of asymptomatic bacteriuria may lead to an erroneous assumption that a UTI is the cause of an acute change of status, hence failing to detect or delaying the timelier detection of 5 signs and symptoms likely indicative of uncomplicated cystitis. These include dysuria, and one or more of the following: frequency, urgency, supra-pubic pain or gross hematuria” (AMDA, 2019).
2018 American Academy of Pediatrics-Section on Nephrology (ASPN) and the American Society of Pediatric Nephrology (AAP)
The AAP Section on Nephrology and the ASPN issued a joint Choosing Wisely recommendation stating, “Avoid ordering follow-up urine cultures after treatment for an uncomplicated urinary tract infection (UTI) in patients that show evidence of clinical resolution of infection. Studies have shown that clinical resolution of infection is adequate for determining effectiveness of antibiotic therapy after treatment for a UTI” (AAP & ASPN, 2018).
2016 American Academy of Pediatrics
The AAP updated their Choosing Wisely recommendation in 2016: “Avoid the use of surveillance cultures for the screening and treatment of asymptomatic bacteriuria.” There is no evidence that surveillance urine cultures or treatment of asymptomatic bacteriuria is beneficial. Surveillance cultures are costly and produce both false positive and false negative results. Treatment of asymptomatic bacteriuria is harmful and increases exposure to antibiotics, which is a risk factor for subsequent infections with a resistant organism. This also results in the overall use of antibiotics in the community and may lead to unnecessary imaging” (AAP, 2016).
2019 Society for Healthcare Epidemiology of America (SHEA)
The SHEA recommendation in Choosing Wisely is more encompassing: “Don’t perform cultures (e.g., urine, blood, sputum cultures) or test for C. difficile unless patients have signs or symptoms of infection. Tests can be falsely positive leading to over diagnosis and overtreatment. Although important for diagnosing disease when used in patients with appropriate signs or symptoms, these tests often are positive when an infection is not present. For example, in the absence of signs or symptoms, a positive blood culture may represent contamination, a positive urine culture could represent asymptomatic bacteriuria, and a positive test for C. difficile could reflect colonization. There are no perfect tests for these or most infections. If these tests are used in patients with low likelihood of infection, they will result in more false positive tests than true positive results, which will lead to treating patients without infection and exposing them to risks of antibiotics without benefits of treating an infection” (SHEA, 2019).
European Association of Urology (EAU)
The EAU in 2021 released an update to their extensive 2020 guidelines concerning urological infections. In 2022 the guidelines were updated with minor changes. With respect to asymptomatic bacteriuria, they state (all with a ‘Strong’ strength of rating), “Do not screen or treat asymptomatic bacteriuria in the following conditions:
- Women without risk factors;
- Patients with well-regulated diabetes mellitus;
- Post-menopausal [individuals];
- Elderly institutionalised patients;
- Patients with dysfunctional and/or reconstructed lower urinary tracts;
- Patients with renal transplants;
- Patients prior to arthroplasty surgeries;
- Patients with recurrent urinary tract infections.”
They do recommend with a "Strong" rating to “screen for and treat asymptomatic bacteriuria prior to urological procedures breaching the mucosa” and a "Weak" rating to “screen for and treat asymptomatic bacteriuria in pregnant [individuals] with standard short course treatment.” They do recommend to “diagnose recurrent UTI by urine culture” with a ‘Strong’ rating. Please note that recurrent UTI indicates that the occurrences are symptomatic. It is further specified that “A urine culture must therefore be taken prior to such interventions”.
With respect to uncomplicated cystitis, they give a "Strong" rating to only perform urine culture analysis “in the following situations:
- Suspected acute pyelonephritis;
- Symptoms that do not resolve or recur within four weeks after the completion of treatment;
- Women who present with atypical symptoms;
- Pregnant [individuals].”
The EAU gives a ‘Weak’ recommendation to “use urine dipstick testing for diagnosis of acute uncomplicated cystitis.”
In cases of uncomplicated pyelonephritis, the EAU recommends with a ‘Strong’ rating to “perform urinalysis (e.g., using the dipstick method), including the assessment of white and red blood cells and nitrite, for routine diagnosis” and to “perform urine culture and antimicrobial susceptibility testing in patients with pyelonephritis.”
The EAU defines complicated UTI (cUTI) as occurring “in an individual in whom factors related to the host (e.g., underlying diabetes or immunosuppression) or specific anatomical or functional abnormalities related to the urinary tract (e.g., obstruction, incomplete voiding due to detrusor muscle dysfunction) are believed to result in an infection that will be more difficult to eradicate than an uncomplicated infection.” Other factors associated with cUTIs include vesicoureteral reflux, recent history of instrumentation, UTI in males, pregnancy, and healthcare-associated infections. “Laboratory urine culture is the recommended method to determine the presence or absence of clinically significant bacteriuria in patients suspected of having a cUTI.”
For catheter-associated UTIs (CAUTI), the EAU recommends with "Strong" ratings to “not carry out routine urine culture in asymptomatic catheterised patients,” to “not use pyuria as sole indicator for catheter-associated UTI,” and to “not use the presence or absence of odorous or cloudy urine alone to differentiate catheter-associated asymptomatic bacteriuria from catheter-associated UTI.”
In cases of urethritis, the EAU states that “Clinicians should always perform point-of-care diagnostics (e.g., Gram staining, first-void urine with microscopy, leukocyte esterase testing) if available to obtain objective evidence of urethral inflammation and to guide treatment … men who meet the criteria for urethritis should be tested for C. trachomatis, M. genitalium and N. gonorrhoeae with nucleic acid amplification tests (NAAT), even if point-of-care tests are negative for gonorrhoeae … N. gonorrhoeae and chlamydia cultures are mainly to evaluate treatment failures and monitor developing resistance to current treatment.” With a "Strong" rating, they recommend:
- “Perform a gram stain of urethral discharge or a urethral smear to preliminarily diagnose gonococcal urethritis.”
- “Perform a validated nucleic acid amplification tests on a first-void urine sample or urethral smear to prior to empirical treatment to diagnose chlamydial and gonococcal infections.”
- “Perform a urethral swab culture, prior to initiation of treatment, in patients with a positive NAAT for gonorrhoea to assess the antimicrobial resistance profile of the infective strain.”
- “Use a pathogen directed treatment based on local resistance data.”
For urosepsis, the EAU strongly recommends to “Take a urine culture and two sets of blood cultures before starting antimicrobial treatment.”
For the diagnosis and disease management of bacterial prostatitis (BP), the EAU recommends with a "Strong" rating to “perform the Meares and Stamey 2- or 4-glass test in patients with [chronic bacterial prostatitis (CBP)].” They only give a "Weak" rating in the use of the urine dipstick test and blood culture with a total blood count for acute bacterial prostatitis (ABP). They also give a "Weak" rating to their recommendation to “not routinely perform microbiological analysis of the ejaculate alone to diagnose CBP;” however, they give a "Strong" recommendation to “treat acute bacterial prostatitis according to the recommendations for complicated UTIs” where they recommend a laboratory urine culture.
The EAU’s recommendation in cases of suspected acute infective epididymitis (with a "Strong" rating) is “to obtain a mid-stream urine and a first-voided urine for pathogen identification by culture and nucleic acid amplification test.” It should be noted that, if the acute scrotal pain and/or swelling is due to suspected torsion, then a urine culture is not necessary. In that case, “urgent surgical exploration” is recommended instead (Bonkat et al., 2022).
World Health Organization (WHO)
The WHO recommendations on antenatal care for a positive pregnancy experience in 2016 does include a recommendation to test for asymptomatic bacteriuria (ASB) in pregnant individuals. “Midstream urine culture is the recommended method for diagnosing asymptomatic bacteriuria (ASB) in pregnancy. In settings where urine culture is not available, the onsite midstream urine Gram-staining is recommended over the use of dipstick tests as the method for diagnosing ASB in pregnancy.” They do make note of the amount of time a urine culture takes (up to 7 days) but state that it is “the gold standard.” The concern of ASB in pregnancy is because “ASB is associated with an increased risk of preterm birth” (WHO, 2016).
Canadian Paediatric Society (CPS)
In 2014, the CPS issued their position statement titled Urinary tract infection in infants and children: Diagnosis and management and reaffirmed their statement in 2020. Their recommendations are for children > 2 months old. They recommend that “infants from two to 36 months of age with a fever of > 39◦C and no other source for fever on history or physical examination … should have urine collected for urinalysis. Unless this test is completely normal, they should then have urine collected by catheter or suprapubic aspirate [SPA] sent for culture.” Currently, CPS notes this statement as inapplicable for infants under 2 months of age (Robinson et al., 2020).
If the child has been toilet-trained, then the urine sample can be collected midstream in lieu of the catheter. “Children with possible UTI who require antibiotic treatment immediately for other indications, such as suspected bacteremia, should have urine collected for urinalysis, microscopy, and culture.” Again, this sample should be obtained via either catheterization or SPA unless the child has been toilet-trained. They also state that “urine collection must occur before starting antibiotics because a single dose of an effective antibiotic rapidly sterilizes the urine” (Robinson et al., 2020).
American Academy of Pediatrics (AAP)
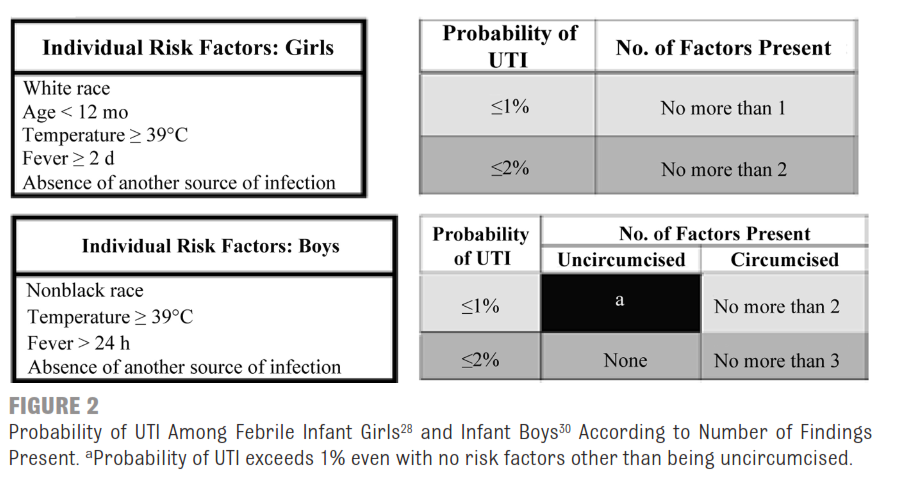
The AAP issued guidelines for UTIs in children 2 to 24 months of age in 2011, which were reaffirmed in 2016. With an “A” grade for evidence quality and a strong recommendation, they issued their Action Statement 1: “If a clinician decides that a febrile infant with no apparent source for the fever requires antimicrobial therapy to be administered because of ill appearance or another pressing reason, the clinician should ensure that a urine specimen is obtained for both culture and urinalysis before an antimicrobial agent is administered; the specimen needs to be obtained through catheterization or SPA, because the diagnosis of UTI cannot be established reliably through culture of urine collected in a bag.” For instances where the clinician believes that the febrile child does not warrant immediate antimicrobial therapy, the AAP in Action Statement 2 (strong recommendation; “A” grade of evidence) the following: (Action Statement 2a) “If the clinician determines the febrile infant to have a low likelihood of UTI [in Table below] then the clinical follow-up monitoring without testing is sufficient.” In Action Statement 2b, the AAP states: “If the clinician determines that the febrile infant is not in a low-risk group [in Table below], then there are 2 choices. Option 1 is to obtain a urine specimen through catheterization or SPA for culture and urinalysis. Option 2 is to obtain a urine specimen through the most convenient means and to perform a urinalysis. If the urinalysis results suggest a UTI (positive leukocyte esterase test results or nitrite test or microscopic analysis results positive for leukocytes or bacteria), then a urine specimen should be obtained through catheterization or SPA and cultures; if urinalysis of fresh (< 1 hour since void) urine yields negative leukocyte esterase and nitrite test results, then it is reasonable to monitor the clinical course without initiating anti-microbial therapy, recognizing that negative urinalysis results do not rule out a UTI with certainty.” The table below from (Roberts, 2011) depicts the level of risk factors separated by gender.
Canadian Urological Association (CUA)
The CUA Guidelines for the diagnosis and management of recurrent urinary tract infection in women contains an algorithm for a “female without a prior history of structural or functional abnormalities of the urinary tract presenting with 3 or more UTIs in 12 months” that requires a urine culture during a time when the patient is symptomatic followed by a urine culture two weeks after initiating treatment with sensitivity-adjusted antibiotics (Level 4 evidence, Grade C recommendation [Recommendation 2c]). In doing so, this “may aid in confirming the diagnosis of UTI, as well as guiding further specialist evaluation and management.” For recurrent uncomplicated UTI, “culture and sensitivity analysis should be performed at least once while the patient is symptomatic …. A midstream urine bacterial count of 1 X 105 CFU/L should be considered a positive culture while the patient is symptomatic.” For patients that choose an option of "self-start antibiotic" therapy, “it is not necessary to culture the urine after UTI self-diagnosis since there is a 86% to 92% concordance between self-diagnosis and urine culture in an appropriately selected patient population. Patients are advised to contact a health care provider if symptoms do not resolve within 48 hours for treatment based on culture and sensitivity” (Dason et al., 2011).
American Urological Association (AUA)
The AUA issued a white paper in 2014 concerning CAUTIs. In the white paper, they refer to the use of the National Surgical Quality Improvement Program (NSQIP) definition of UTIs, which does reference the use of urine culture. It should be noted, however, that this definition requires at least a minimum of one of the following symptoms: fever (> 38◦C), urgency, frequency, dysuria, or suprapubic tenderness. They too refer to the 2009 IDSA guidelines concerning CAUTIs as well as those of the EAU. They state that there are “no consistent guidelines are available on how to obtain urine for culture from chronically catheterized patients, or what constitutes true urinary tract infection versus asymptomatic bacteriuria.” They make note of a study concerning the possible cost-effectiveness of the use of dipsticks to screen asymptomatic ICU patients for CAUTIs. They conclude, “however, as previously discussed, screening of asymptomatic patients may not be warranted, and treatment is usually not recommended in these cases” (Averch et al., 2014).
The AUA released guidelines for primary vesicoureteral reflux in children and recommend “Urinalysis for proteinuria and bacteriuria is recommended. If the urinalysis indicates infection, a urine culture and sensitivity is recommended.” The AUA also recommends urinalysis annually as part of the follow-up procedure (AUA, 2017).
The AUA published an update to their 2012 guideline on Urologic Procedures and Antimicrobial Prophylaxis, termed a “Best Practice Statement.”
The AUA recommends that “Prior to any urologic procedure, evaluation of a patient’s urinary tract symptoms suggestive of a UTI should include a simple dipstick, laboratory performed microscopy, and/or formal culture.”
The AUA also states that “Positive microscopy findings should be confirmed with a culture for antimicrobial sensitivities in the perioperative setting where the risk of an SSI is high and targeted antimicrobial treatment may be required. Urine culture should not be performed without an accompanying urine microscopy due to common sample contamination as well as bacterial colonization” (Lightner et al., 2020).
National Institute for Health and Care Excellence (NICE)
NICE recommends against using dipstick testing to diagnose UTIs in adults with urinary catheters. However, NICE states that patients with a UTI not responding to initial antibiotic treatment should have a urine culture (NICE, 2015).
NICE also recommended the following populations of children for a urine culture:
- in infants and children who are suspected to have acute pyelonephritis/upper urinary tract infection
- in infants and children with a high to intermediate risk of serious illness
- in infants under 3 months
- in infants and children with a positive result for leukocyte esterase or nitrite
- in infants and children with recurrent UTI
- in infants and children with an infection that does not respond to treatment within 24 – 48 hours, if no sample has already been sent
- when clinical symptoms and dipstick tests do not correlate (NICE, 2018)
American Urological Association (AUA)/Canadian Urological Association (CUA)/Society of Urodynamics, Female Pelvic Medicine & Urogenital Reconstruction (SUFU)
These joint guidelines focus on “recurrent episodes of uncomplicated cystitis in women” and are not intended for “pregnant [individuals], patients who are immunocompromised, those with anatomic or functional abnormalities of the urinary tract, women with rUTIs due to self-catheterization or indwelling catheters, or those exhibiting signs or symptoms of systemic bacteremia, such as fever and flank pain.” Their recommendations are listed below:
- “Clinicians should obtain urinalysis, urine culture and sensitivity with each symptomatic acute cystitis episode prior to initiating treatment in patients with rUTIs. (Moderate Recommendation; Evidence Level: Grade C)”
- “Clinicians should omit surveillance urine testing, including urine culture, in asymptomatic patients with rUTIs” (Moderate Recommendation; Evidence Level: Grade C)” (Anger et al., 2019).
Infectious Diseases Society of America (IDSA)
These guidelines were intended to update the 2005 IDSA guidelines. Their recommendations for asymptomatic bacteriuria (ASB) are as follows:
- “In infants and children, we recommend against screening for or treating asymptomatic bacteriuria.”
- “In healthy premenopausal, nonpregnant [individuals] or healthy postmenopausal [individuals], we recommend against screening for or treating ASB.”
- “In pregnant [individuals], we recommend screening for and treating ASB.”
- “In older, community-dwelling persons who are functionally impaired, we recommend against screening for or treating ASB.”
- “In older persons resident in long-term care facilities, we recommend against screening for or treating ASB.”
- “In patients with diabetes, we recommend against screening for or treating ASB.”
- “In renal transplant recipients who have had renal transplant surgery > 1 month prior, we recommend against screening for or treating ASB.”
- “In patients with nonrenal solid organ transplant (SOT), we recommend against screening for or treating ASB.”
- “In patients with high-risk neutropenia (absolute neutrophil count < 100 cells/mm3, ≥ 7 days’ duration following chemotherapy), we make no recommendation for or against screening for or treatment of ASB.”
- “In patients with spinal cord injury (SCI), we recommend against screening for or treating ASB.”
- “In patients with a short-term indwelling urethral catheter (< 30 days), we recommend against screening for or treating ASB.”
- “In patients undergoing elective nonurologic surgery, we recommend against screening for or treating ASB.”
- “In patients who will undergo endoscopic urologic procedures associated with mucosal trauma, we recommend screening for and treating ASB prior to surgery.”
The guideline also states that it has been reviewed and endorsed by the following societies: “the Society of Healthcare Epidemiology of America, Pediatric Infectious Diseases Society, American College of Obstetrics and Gynecology, Association of Medical Microbiology and Infectious Diseases Canada, European Society of Clinical Microbiology and Infectious Diseases, European Association of Urology, and the American Urological Association” (Nicolle et al., 2019).
U.S. Preventive Services Task Force (USPSTF)
The USPSTF recommends screening for “asymptomatic bacteriuria using urine culture in pregnant persons,” but recommends against “screening for asymptomatic bacteriuria in nonpregnant adults” (USPSTF, 2019).
American Society of Transplantation Infectious Diseases
These guidelines focus on UTIs within the kidney transplant (KT) population. The recommendations are listed below:
“We recommend against routinely collecting urine culture or treating bacteriuria in asymptomatic KT patients more than two months after KT.”
“If screening asymptomatic KT recipients any time in the post-transplant period and A[S]B [asymptomatic bacteriuria] is found, a second urine culture (minimizing risk of contamination) should be collected and reviewed prior to decision about whether or not to treat AB. We strongly recommend observation without treatment of asymptomatic KT patients recipients who show clearance of the initial bacteriuria or development of different organism in the urine” (Goldman & Julian, 2019).
Canadian Task Force on Preventive Health Care
This guideline focuses on screening for asymptomatic bacteriuria during pregnancy.
“We recommend screening pregnant [individuals]once during the first trimester with urine culture for asymptomatic bacteriuria”, which applies to “pregnant [individuals] who are not experiencing symptoms of a urinary tract infection and are not at increased risk for asymptomatic bacteriuria.” However, the guideline remarks that this recommendation is “weak” with “very-low” quality of evidence (Moore et al., 2018).
Choosing Wisely Canada
The Association of Medical Microbiology and Infectious Diseases Canada recommends against collecting “urine specimens for culture from adults who lack symptoms localizing to the urinary tract or fever unless they are pregnant or undergoing genitourinary instrumentation where mucosal bleeding is expected.” The guideline further recommends that laboratories “consider supplementing educational efforts to reduce collection of urine cultures from asymptomatic patients with analytical interventions that reduce processing of low-value specimens” (Association of Medical Microbiology and Infectious Diseases Canada, 2021).
Table of Terminology
|
Term |
Definition |
|
AAP |
American Academy of Pediatrics |
|
ABIM |
American Board of Internal Medicine |
|
ABP |
Acute bacterial prostatitis |
|
ACOG |
American College of Obstetricians and Gynecologists |
|
AMDA |
The Society for Post-Acute and Long-Term Care Medicine |
|
ARESC |
Antimicrobial Resistance Epidemiological Survey on Cystitis |
|
ASB |
Asymptomatic bacteriuria |
|
ASPN |
American Society of Pediatric Nephrology |
|
AUA |
American Urological Association |
|
AUC |
Area under the curve |
|
BP |
Bacterial prostatitis |
|
CAUTI |
Catheter-associated urinary tract infection |
|
CBP |
Chronic bacterial prostatitis |
|
CDC |
Centers for Disease Control and Prevention |
|
CFU |
Colony-forming unit |
|
CLIA ’88 |
Clinical Laboratory Improvement Amendments of 1988 |
|
CMS |
Centers For Medicare and Medicaid |
|
CPS |
Canadian Paediatric Society |
|
CUA |
Canadian Urological Association |
|
cUTI |
Complicated urinary tract infection |
|
DNA |
Deoxyribonucleic acid |
|
DOR |
Diagnostic odds ratio |
|
EAU |
European Association of Urology |
|
EQUC |
Enhanced quantitative urine culture |
|
FDA |
Food and Drug Administration |
|
FUM |
Female urinary microbiota |
|
ICU |
Intensive care unit |
|
IDSA |
Infectious Diseases Society of America |
|
KT |
Kidney transplant |
|
LCD |
Local coverage determination |
|
LDT |
Laboratory-developed test |
|
MRSA |
Methicillin-Resistant Staphylococcus Aureus |
|
MSSA |
Methicillin-Sensitive Staphylococcus Aureus |
|
NAAT |
Nucleic acid amplification test |
|
NCD |
National coverage determination |
|
NICE |
National Institute for Health and Care Excellence |
|
NSQIP |
National Surgical Quality Improvement Program |
|
OR |
Odds ratio |
|
PA |
Prior authorization |
|
PCR |
Polymerase chain reaction |
|
RNA |
Ribonucleic acid |
|
rUTIs |
Recurrent urinary tract infection |
|
SCI |
Spinal cord injury |
|
SHEA |
Society for Healthcare Epidemiology of America |
|
SOT |
Solid organ transplant |
|
SPA |
Suprapubic aspiration |
|
SSI |
Surgical site infection |
|
SUFU |
Society Of Urodynamics, Female Pelvic Medicine & Urogenital Reconstruction |
|
UA |
Urinalysis |
|
USPSTF |
United States Preventive Services Task Force |
|
UTI |
Urinary tract infection |
|
WHO |
World Health Organization |
References
-
AAP. (2016, July 13). Avoid the use of surveillance cultures for the screening and treatment of asymptomatic bacteriuria. ABIM. Retrieved 06/20/2018 from http://www.choosingwisely.org/clinician-lists/american-academy-pediatrics-surveillance-cultures-to-screen-and-treat-asymptomatic-bacteruria/
-
AAP, & ASPN. (2018, July 16). Avoid ordering follow-up urine cultures after treatment for an uncomplicated urinary tract infection (UTI) in patients that show evidence of clinical resolution of infection. ABIM. Retrieved 04/19/2019 from http://www.choosingwisely.org/clinician-lists/aap-aspn-follow-up-urine-cultures-after-treatment-for-uncomplicated-uti/
-
AMDA. (2019). Don’t obtain urine tests until clinical criteria are met. ABIM. http://www.choosingwisely.org/clinician-lists/amda-urine-cultures/
-
Anger, J., Lee, U., Ackerman, L., Chou, R., Chughtai, B., Quentin Clemens, J., Hickling, D., Kapoor, A., Kenton, K. S., Kaufman, M. R., Rondanina, M. A., Stapleton, A., Stothers, L., & Chai, T. C. (2019, April). Recurrent Uncomplicated Urinary Tract Infections in Women: AUA/CUA/SUFU Guideline. American Urological Association. Retrieved 04/03 from https://www.cua.org/system/files/Guidelines/rUTI-guideline.pdf
-
Aroutcheva, A., Gariti, D., Simon, M., Shott, S., Faro, J., Simoes, J. A., Gurguis, A., & Faro, S. (2001). Defense factors of vaginal lactobacilli. Am J Obstet Gynecol, 185(2), 375-379. https://doi.org/10.1067/mob.2001.115867
-
Association of Medical Microbiology and Infectious Diseases Canada. (2021). Five Tests and Treatments to Question in Medical Microbiology and Infectious Diseases. https://choosingwiselycanada.org/recommendation/medical-microbiology/
-
AUA. (2017). Management and Screening of Primary Vesicoureteral Reflux in Children. https://www.auanet.org/guidelines/vesicoureteral-reflux-(2010-amended-2017)
-
Averch, T. D., Stoffel, J., Goldman, H. B., Griebling, T. L., Lerner, L., Newman, D. K., Peterson, A. C., Bertsch, J., Hoogland, M., Hubbard, H., Pope, S., Shertz Wall, C., & Yoffe, M. (2014, 2014). Catheter-Associated Urinary Tract Infections: Definitions and Significance in the Urologic Patient. American Urological Association. Retrieved 06/21/2018 from http://www.auanet.org/guidelines/catheter-associated-urinary-tract-infections
-
Birnie, K., Hay, A. D., Wootton, M., Howe, R., MacGowan, A., Whiting, P., Lawton, M., Delaney, B., Downing, H., Dudley, J., Hollingworth, W., Lisles, C., Little, P., O'Brien, K., Pickles, T., Rumsby, K., Thomas-Jones, E., Van der Voort, J., Waldron, C. A., . . . Sterne, J. A. (2017). Comparison of microbiological diagnosis of urinary tract infection in young children by routine health service laboratories and a research laboratory: Diagnostic cohort study. (1932-6203 (Electronic)).
-
Bonkat, G., Bartoletti, R., Bruyère, R., Cai, T., Geerlings, S. E., Koves, B., Schubert, S., Pilatz, A., Veeratterapillay, R., & Wagenlehner, F. M. E. (2022, 2018). European Association of Urology (EAU) Guidelines on Urological Infections Uroweb. Retrieved 06/20/2018 from https://uroweb.org/guidelines/urological-infections
-
Brubaker, L., & Wolfe, A. (2016). The urinary microbiota: a paradigm shift for bladder disorders? Curr Opin Obstet Gynecol, 28(5), 407-412. https://doi.org/10.1097/gco.0000000000000298
-
Bruyere, F., d'Arcier, B. F., Boutin, J. M., & Haillot, O. (2010). Is urine culture routinely necessary before prostate biopsy? Prostate Cancer Prostatic Dis, 13(3), 260-262. https://doi.org/10.1038/pcan.2010.8
-
Cantey, J. B., Gaviria-Agudelo, C., McElvania TeKippe, E., & Doern, C. D. (2015). Lack of clinical utility of urine gram stain for suspected urinary tract infection in pediatric patients. Journal of Clinical Microbiology, 53(4), 1282-1285. https://doi.org/10.1128/JCM.00045-15
-
CDC. (2019). Urinary Tract Infection. https://www.cdc.gov/antibiotic-use/community/for-patients/common-illnesses/uti.html
-
Cooper, J., Raeburn, A., Hamilton-Miller, J. M., & Brumfitt, W. (1992). Nitrite test for bacteriuria detection. Br J Gen Pract, 42.
-
Cope, M., Cevallos, M. E., Cadle, R. M., Darouiche, R. O., Musher, D. M., & Trautner, B. W. (2009). Inappropriate treatment of catheter-associated asymptomatic bacteriuria in a tertiary care hospital. Clin Infect Dis, 48(9), 1182-1188. https://doi.org/10.1086/597403
-
Coussement, J., Scemla, A., Hougardy, J. M., Sberro-Soussan, R., Amrouche, L., Catalano, C., Johnson, J. R., & Abramowicz, D. (2019). Prevalence of asymptomatic bacteriuria among kidney transplant recipients beyond two months post-transplant: A multicenter, prospective, cross-sectional study. PLoS One, 14(9), e0221820. https://doi.org/10.1371/journal.pone.0221820
-
Dason, S., Dason, J. T., & Kapoor, A. (2011). Guidelines for the diagnosis and management of recurrent urinary tract infection in women. Can Urol Assoc J, 5(5), 316-322. https://doi.org/10.5489/cuaj.11214
-
Devillé, W. L. J. M., Yzermans, J. C., van Duijn, N. P., Bezemer, P. D., van der Windt, D. A. W. M., & Bouter, L. M. (2004). The urine dipstick test useful to rule out infections. A meta-analysis of the accuracy. BMC Urology, 4(1), 4. https://doi.org/10.1186/1471-2490-4-4
-
Ducharme, J., Neilson, S., & Ginn, J. L. (2007). Can urine cultures and reagent test strips be used to diagnose urinary tract infection in elderly emergency department patients without focal urinary symptoms? Cjem, 9(2), 87-92.
-
Eliacik, K., Kanik, A., Yavascan, O., Alparslan, C., Kocyigit, C., Aksu, N., & Bakiler, A. R. (2016). A Comparison of Bladder Catheterization and Suprapubic Aspiration Methods for Urine Sample Collection From Infants With a Suspected Urinary Tract Infection. Clin Pediatr (Phila), 55(9), 819-824.
-
Fontserè, S., Infante-Domínguez, C., Suárez-Benjumea, A., Suñer-Poblet, M., González-Corvillo, C., Martín-Gutiérrez, G., Bernal, G., Pachón, J., Pachón-Ibáñez, M. E., & Cordero, E. (2021). Impact of Treating Asymptomatic Bacteriuria in Kidney Transplant Recipients: A Prospective Cohort Study. Antibiotics (Basel, Switzerland), 10(2), 218. https://doi.org/10.3390/antibiotics10020218
-
Goldman, J. D., & Julian, K. (2019). Urinary tract infections in solid organ transplant recipients: Guidelines from the American Society of Transplantation Infectious Diseases Community of Practice. Clin Transplant, 33(9), e13507. https://doi.org/10.1111/ctr.13507
-
Graham, J., & Galloway, A. (2001). ACP Best Practice No 167. Journal of Clinical Pathology, 54(12), 911-919. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1731340/
-
Harding, G. K., Zhanel, G. G., Nicolle, L. E., & Cheang, M. (2002). Antimicrobial treatment in diabetic women with asymptomatic bacteriuria. N Engl J Med, 347(20), 1576-1583. https://doi.org/10.1056/NEJMoa021042
-
Hooton, T. M., & Gupta, K. (2021, March 19). Acute complicated urinary tract infection (including pyelonephritis) in adults. Wolters Kluwer. https://www.uptodate.com/contents/acute-complicated-urinary-tract-infection-including-pyelonephritis-in-adults
-
Lightner, D. J., Wymer, K., Sanchez, J., & Kavoussi, L. (2020). Best Practice Statement on Urologic Procedures and Antimicrobial Prophylaxis. J Urol, 203(2), 351-356. https://doi.org/10.1097/ju.0000000000000509
-
Meyrier, A. (2021, July 12). Sampling and evaluation of voided urine in the diagnosis of urinary tract infection in adults. Wolters Kluwer. https://www.uptodate.com/contents/sampling-and-evaluation-of-voided-urine-in-the-diagnosis-of-urinary-tract-infection-in-adults
-
Moore, A., Doull, M., Grad, R., Groulx, S., Pottie, K., Tonelli, M., Courage, S., Garcia, A. J., & Thombs, B. D. (2018). Recommendations on screening for asymptomatic bacteriuria in pregnancy. Cmaj, 190(27), E823-e830. https://doi.org/10.1503/cmaj.171325
-
NICE. (2015, June 11). Urinary tract infections in adults. https://www.nice.org.uk/guidance/qs90/chapter/List-of-quality-statements
-
NICE. (2018, October 31). Urinary tract infection in under 16s: diagnosis and management. https://www.nice.org.uk/guidance/cg54/resources/urinary-tract-infection-in-under-16s-diagnosis-and-management-pdf-975507490501
-
Nicolle, L. E., Gupta, K., Bradley, S. F., Colgan, R., DeMuri, G. P., Drekonja, D., Eckert, L. O., Geerlings, S. E., Koves, B., Hooton, T. M., Juthani-Mehta, M., Knight, S. L., Saint, S., Schaeffer, A. J., Trautner, B., Wullt, B., & Siemieniuk, R. (2019). Clinical Practice Guideline for the Management of Asymptomatic Bacteriuria: 2019 Update by the Infectious Diseases Society of America. Clin Infect Dis, 68(10), e83-e110. https://doi.org/10.1093/cid/ciy1121
-
Petty, L. A., Vaughn, V. M., Flanders, S. A., Malani, A. N., Conlon, A., Kaye, K. S., Thyagarajan, R., Osterholzer, D., Nielsen, D., Eschenauer, G. A., Bloemers, S., McLaughlin, E., & Gandhi, T. N. (2019). Risk Factors and Outcomes Associated With Treatment of Asymptomatic Bacteriuria in Hospitalized Patients. JAMA Intern Med. https://doi.org/10.1001/jamainternmed.2019.2871
-
Price, T. K., Dune, T., Hilt, E. E., Thomas-White, K. J., Kliethermes, S., Brincat, C., Brubaker, L., Wolfe, A. J., Mueller, E. R., & Schreckenberger, P. C. (2016). The Clinical Urine Culture: Enhanced Techniques Improve Detection of Clinically Relevant Microorganisms. Journal of Clinical Microbiology, 54(5), 1216-1222. https://doi.org/10.1128/JCM.00044-16
-
Roberts, K. B. (2011). Urinary tract infection: clinical practice guideline for the diagnosis and management of the initial UTI in febrile infants and children 2 to 24 months. Pediatrics, 128(3), 595-610. https://doi.org/10.1542/peds.2011-1330
-
Robinson, J. L., Finlay, J. C., Lang, M. E., Bortolussi, R., CPS, CPC, & IDIC. (2020). Urinary tract infections in infants and children: Diagnosis and management. Canadian Paediatric Society. https://www.cps.ca/en/documents/position/urinary-tract-infections-in-children
-
Schito, G. C., Naber Kg Fau - Botto, H., Botto H Fau - Palou, J., Palou J Fau - Mazzei, T., Mazzei T Fau - Gualco, L., Gualco L Fau - Marchese, A., & Marchese, A. (2009). The ARESC study: an international survey on the antimicrobial resistance of pathogens involved in uncomplicated urinary tract infections. Int J Antimicrob Agents, 34(5), 407-413.
-
Schmiemann, G., Kniehl, E., Gebhardt, K., Matejczyk, M. M., & Hummers-Pradier, E. (2010). The Diagnosis of Urinary Tract Infection: A Systematic Review. Deutsches Ärzteblatt International, 107(21), 361-367. https://doi.org/10.3238/arztebl.2010.0361
-
SHEA. (2019, December 2). Don't perform urinalysis, urine culture, blood culture or C. difficile testing unless patients have signs or symptoms of infection. ABIM. http://www.choosingwisely.org/clinician-lists/shea-urinalysis-urine-culture-blood-culture-or-c-difficile-testing/
-
USPSTF. (2019). Screening for Asymptomatic Bacteriuria in Adults: US Preventive Services Task Force Recommendation Statement. JAMA, 322(12), 1188-1194. https://doi.org/10.1001/jama.2019.13069
-
WHO. (2016). WHO Guidelines Approved by the Guidelines Review Committee. In WHO Recommendations on Antenatal Care for a Positive Pregnancy Experience. World Health Organization Copyright (c) World Health Organization 2016. https://apps.who.int/iris/bitstream/handle/10665/250796/9789241549912-eng.pdf?sequence=1
-
Wojno, K. J., Baunoch, D., Luke, N., Opel, M., Korman, H., Kelly, C., Jafri, S. M. A., Keating, P., Hazelton, D., Hindu, S., Makhloouf, B., Wenzler, D., Sabry, M., Burks, F., Penaranda, M., Smith, D. E., Korman, A., & Sirls, L. (2020). Multiplex PCR Based Urinary Tract Infection (UTI) Analysis Compared to Traditional Urine Culture in Identifying Significant Pathogens in Symptomatic Patients. Urology, 136, 119-126. https://doi.org/10.1016/j.urology.2019.10.018
Coding Section
|
Code |
Number |
Description |
|
CPT |
87077 |
Culture, bacterial; aerobic isolate, additional methods required for definitive identification, each isolate |
|
|
87086 |
Culture, bacterial; quantitative colony count, urine |
|
|
87088 |
Culture, bacterial; with isolation and presumptive identification of each isolate, urine |
|
|
87140 |
Culture, typing; immunofluorescent method, each antiserum |
| 87147 | Culture, typing; immunologic method, other than immunofluorescence (eg, agglutination grouping), per antiserum | |
|
|
87149 |
Culture, typing; identification by nucleic acid (DNA or RNA) probe, direct probe technique, per culture or isolate, each organism probed |
|
|
87181 |
Susceptibility studies, antimicrobial agent; agar dilution method, per agent (eg, antibiotic gradient strip) |
Procedure and diagnosis codes on Medical Policy documents are included only as a general reference tool for each policy. They may not be all-inclusive.
This medical policy was developed through consideration of peer-reviewed medical literature generally recognized by the relevant medical community, U.S. FDA approval status, nationally accepted standards of medical practice and accepted standards of medical practice in this community, Blue Cross Blue Shield Association technology assessment program (TEC) and other nonaffiliated technology evaluation centers, reference to federal regulations, other plan medical policies, and accredited national guidelines.
"Current Procedural Terminology © American Medical Association. All Rights Reserved"
History From 2018 Forward
|
07/28/2022 |
Annual review, updating policy for clarity and pronoun update. No change to policy intent. Updating description, rationale and references. |
|
07/12/2021 |
Annual review, no change to policy intent. Updating policy verbiage to remove urinalysis testing for clarity. Updating coding, description, rationale and references. |
|
07/01/2020 |
Annual review, no change to policy intent. Updating coding. |
|
07/12/2019 |
Annual review, reordering policy criteria and adding verbiage regarding follow up testing. |
|
09/04/2018 |
This Policy has an Effective Date of 12/01/2018. |
|
08/14/2018 |
New Policy |